| Size | Price | Stock | Qty |
|---|---|---|---|
| 500mg |
|
||
| 1g |
|
||
| 2g |
|
||
| 5g |
|
||
| 10g |
|
||
| 25g |
|
||
| 50g |
|
||
| Other Sizes |
































Purity: ≥98%
Phenylephrine HCl (Metaoxedrine chloride; NCIc-55641; NCI c55641; Neosympatol; Oftalfrine; Mezaton; Neo Synephrine; Neo-Synephrine), the hydrochloride salt of Phenylephrine, is a potent and selective α1-adrenergic receptor agonist that is primarily used as a decongestant. It is a nasal decongestant, mydriatic, and cardiotonic agent.
| Targets |
α adrenergic receptor
α1-adrenoceptor (agonist, Ki = 0.1 μM) [1][2] |
|---|---|
| ln Vitro |
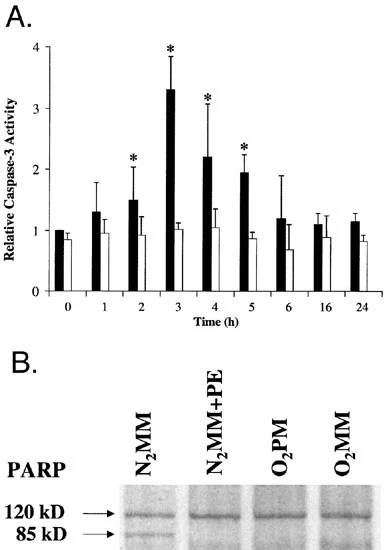
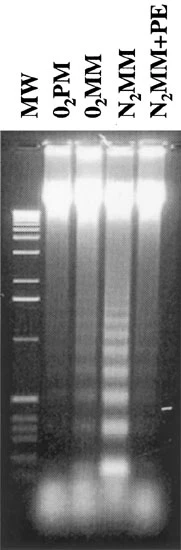
In vitro activity: Phenylephrine causes PKC-epsilon to translocate quickly (EC50 = 0.9 mM), but less of the soluble fraction is lost than with ET-1. When phentolamine is added, the dose-dependent increase in contractile force of the hyperpermeable cells caused by phenylephrine at pCa 7 can be reversed. Additionally, phenylephrine shields cardiomyocytes from hypoxia and serum deprivation treatments that follow for a full day. Phenylephrine prevents the down-regulation of Bcl-2 and Bcl-X mRNA/protein and induces hypertrophic growth. The caspase-9 peptidic inhibitor LEHD-fmk mimics phenylephrine-mediated protection, while the wortmannin inhibitor phosphoinositol 3-kinase (PI 3-kinase) abrogates it. Phosphoinositide (PI) hydrolysis, cell proliferation, and the expression of multiple genes—including atrial natriuretic factor (ANF)—that are frequently linked to cardiac hypertrophy are all stimulated by phenylephrine. The synthesis and proliferation of hepatocyte DNA induced by HGF is significantly enhanced by phenylephrine. I(Ca,L) is reversibly increased by phenylephrine (10 mM; n = 40) and its peak I(Ca,L) activation voltage is shifted by -10 mV. Additionally, through IP3-dependent signaling, phenylephrine increases local, subsarcolemmal SR Ca 2+ release. Both IP3-dependent Ca 2+ signaling and PI-3K/Akt stimulation are necessary for phenylephrin-induced NOi release. A combination of 1 mM prazocin, 10 mM L-NIO, 10 mM W-7, 10 mM LY294002, 2 mM H-89, 10 mM ryanodine, 5 mM thapsigargin, 2 mM 2-APB, or 10 mM xestospongin C inhibits phenylephrine-induced NOi release.
Phenylephrine HCl induced concentration-dependent contraction of isolated rabbit aortic smooth muscle via α1-adrenoceptor activation. At 0.01-1 μM, it achieved maximal contraction of ~90% relative to KCl (60 mM) - induced contraction, with an EC50 of 0.08 μM [2][4] It stimulated phospholipase C (PLC) activation and inositol 1,4,5-trisphosphate (IP3) production in rat hepatocytes. Treatment with 1-10 μM for 30 minutes increased IP3 levels by ~2.5-fold, mediating intracellular calcium release [1] In human umbilical vein endothelial cells (HUVECs), Phenylephrine HCl (10-50 μM) induced apoptosis via reactive oxygen species (ROS) generation, with apoptotic rate increasing from ~5% to ~30% at 50 μM [3] It enhanced L-type calcium current (ICa,L) in rat ventricular myocytes. At 1 μM, ICa,L amplitude increased by ~40%, promoting myocardial contractility [6] |
| ln Vivo |
Perfusion of hearts with 100 μM phenylephrine results in a 12-fold activation of two p38-MAPK isoforms that happens quickly (maximum at 10 min). Heart contractility is enhanced by α1-adrenoceptor agonists, like phenylephrine. Neonatal ventricular myocytes' SAPKs and JNKs are also activated by phenylephrine. In rats with high tidal volume ventilation, phenylephrine may enhance the clearance of alveolar fluid and hasten the absorption of pulmonary edema.
In anesthetized rats, intravenous administration of Phenylephrine HCl (0.1-1 mg/kg) dose-dependently increased systolic blood pressure by ~15-40% and reduced heart rate by ~10-20% (reflex bradycardia). The pressor effect peaked at 10 minutes and persisted for ~40 minutes [2][5] In conscious dogs, intravenous infusion of Phenylephrine HCl (0.5 μg/kg/min) reduced renal blood flow by ~25% and increased renal vascular resistance by ~30%, without affecting glomerular filtration rate [4] In a rat model of hemorrhagic shock, intravenous Phenylephrine HCl (0.3 mg/kg) restored mean arterial pressure from ~60 mmHg to ~95 mmHg within 5 minutes, improving tissue perfusion [5] |
| Enzyme Assay |
α1-adrenoceptor radioligand binding assay: Prepare membrane homogenates from rat cerebral cortex (α1-adrenoceptor-enriched). Incubate homogenates with [3H]-prazosin (0.5 nM) and various concentrations of Phenylephrine HCl (0.001-10 μM) at 25°C for 90 minutes. Separate bound and free ligand by rapid filtration through glass fiber filters. Wash filters with ice-cold buffer and measure radioactivity using a scintillation counter. Calculate Ki value from competition binding curves [1][2]
|
| Cell Assay |
Rabbit aortic smooth muscle contraction assay: Isolate rabbit aortic segments, cut into 2 mm rings, and mount in organ baths with oxygenated Krebs-Ringer solution at 37°C. Equilibrate for 1 hour, then add Phenylephrine HCl (0.001-10 μM) cumulatively. Record tension changes using an isometric transducer and calculate contraction percentage relative to KCl-induced contraction [2][4]
Rat hepatocyte IP3 production assay: Isolate rat hepatocytes and culture in Williams’ medium E. Treat cells with Phenylephrine HCl (1-10 μM) for 30 minutes. Extract IP3 using acidified methanol and quantify via radioimmunoassay [1] HUVEC apoptosis assay: Culture HUVECs in endothelial cell growth medium until confluent. Treat cells with Phenylephrine HCl (10-50 μM) for 24 hours. Detect apoptosis via Annexin V-FITC/PI double staining and flow cytometry. Measure ROS levels with a fluorescent probe [3] |
| Animal Protocol |
Random number tables are used to randomly assign 170 male Wistar rats into 17 groups (n=10). Induce lung injury, impair active Na+ transport, and reduce lung liquid clearance in rats by administering short-term (40 minutes) high-tidal volume mechanical ventilation. Control rats are those that are not ventilated. A variety of phenylephrine concentrations (10, 1, 0.1, 0.01, and 0.001 μM) are injected into the alveolar space of rats on HVT ventilation in order to show how the drug affects alveolar fluid clearance.
Rats Anesthetized rat hemodynamic assay: Adult male rats are anesthetized with urethane, implanted with femoral artery catheters for blood pressure monitoring, and jugular vein catheters for drug administration. Phenylephrine HCl is dissolved in physiological saline and administered intravenously at 0.1, 0.5, or 1 mg/kg. Systolic/diastolic blood pressure and heart rate are recorded continuously for 1 hour [2][5] Conscious dog renal function assay: Adult dogs are instrumented with renal artery flow probes and arterial catheters. After recovery, Phenylephrine HCl is infused intravenously at 0.5 μg/kg/min for 30 minutes. Renal blood flow, renal vascular resistance, and glomerular filtration rate are measured at baseline and during infusion [4] Rat hemorrhagic shock model: Adult rats are anesthetized, and hemorrhagic shock is induced by withdrawing 30% of blood volume. Phenylephrine HCl (0.3 mg/kg) is administered intravenously, and mean arterial pressure is monitored for 60 minutes to assess hemodynamic recovery [5] |
| ADME/Pharmacokinetics |
Absorption: The oral bioavailability of phenylephrine hydrochloride is low (approximately 4-10% in humans), due to first-pass metabolism by monoamine oxidase (MAO) [5]. Distribution: It is rapidly distributed into tissues, with a volume of distribution (Vdss) of approximately 2-3 L/kg in the human body [5]. Metabolism: It is primarily metabolized in the liver and intestines by MAO and sulfotransferases, producing inactive metabolites [5]. Excretion: The plasma elimination half-life in the human body is approximately 2-3 hours. Approximately 70-80% of the dose is excreted in the urine within 24 hours, and approximately 10-15% is excreted unchanged [5]. Plasma protein binding: The plasma protein binding rate of phenylephrine hydrochloride in the human body is approximately 10-15% [5].
|
| Toxicity/Toxicokinetics |
The acute intravenous LD50 in mice was approximately 20 mg/kg; lethal doses could induce severe hypertension, ventricular arrhythmias, and cerebral hemorrhage [5]. Common adverse reactions in humans included hypertension (occurrence rate of approximately 25%), headache (approximately 18%), reflex bradycardia (approximately 12%), and nasal irritation (approximately 10% with local administration) [2][5]. In a rat subchronic toxicity study (28 days), oral doses up to 50 mg/kg/day showed no significant hepatotoxicity or nephrotoxicity, but mild myocardial hypertrophy occurred at a dose of 50 mg/kg/day [3].
|
| References | |
| Additional Infomation |
Phenylephrine hydrochloride is an odorless, white, microcrystalline powder with a bitter taste. Its pH (1% aqueous solution) is approximately 5. (NTP, 1992)
Phenylephrine hydrochloride is the hydrochloride salt form of phenylephrine, a direct-acting sympathomimetic amine whose chemical structure is related to adrenaline and ephedrine, exhibiting potent vasoconstrictive effects. Phenylephrine is a postsynaptic α-adrenergic receptor agonist that causes vasoconstriction, increases systolic/diastolic blood pressure, induces reflex bradycardia, and increases stroke volume. It is an α-1 adrenergic agonist used as a mydriatic, nasal decongestant, and cardiotonic. See also: Phenylephrine (with active ingredient); Ibuprofen; Phenylephrine hydrochloride (one of the ingredients); Phenylephrine hydrochloride; Topicalcide (ingredient)... See more... Phenylephrine hydrochloride is a selective α1-adrenergic receptor agonist with peripheral vasoconstrictive activity [1][2][4][5] Its mechanism of action includes activating α1-adrenergic receptors to induce smooth muscle contraction (blood vessels, viscera), stimulating PLC-IP3-calcium signal transduction, and regulating myocardial calcium current [1][2][6] Based on its vasoconstrictive effect, it is clinically used to treat acute hypotension, hemorrhagic shock, and nasal congestion (topical preparation) [2][5] High concentrations can induce endothelial cell apoptosis through ROS generation, suggesting that supraphysiological doses may have vascular toxicity [3] Due to low oral bioavailability, intravenous or local administration is the preferred method to improve therapeutic effects; oral preparations require higher doses [5] |
| Molecular Formula |
C9H14CLNO2
|
|
|---|---|---|
| Molecular Weight |
203.67
|
|
| Exact Mass |
203.071
|
|
| Elemental Analysis |
C, 53.08; H, 6.93; Cl, 17.41; N, 6.88; O, 15.71
|
|
| CAS # |
61-76-7
|
|
| Related CAS # |
Phenylephrine-2,4,6-d3 hydrochloride; 1276197-50-2; Phenylephrine; 59-42-7; Phenylephrine-d3 hydrochloride; 1217858-50-8; (S)-Phenylephrine-d6 hydrochloride; Phenylephrine-d6 hydrochloride; 1089675-56-8
|
|
| PubChem CID |
5284443
|
|
| Appearance |
White to off-white solid powder
|
|
| Boiling Point |
341.1ºC at 760 mmHg
|
|
| Melting Point |
143-145 °C(lit.)
|
|
| Flash Point |
163.4ºC
|
|
| Index of Refraction |
-45.5 ° (C=1, H2O)
|
|
| LogP |
1.837
|
|
| Hydrogen Bond Donor Count |
4
|
|
| Hydrogen Bond Acceptor Count |
3
|
|
| Rotatable Bond Count |
3
|
|
| Heavy Atom Count |
13
|
|
| Complexity |
130
|
|
| Defined Atom Stereocenter Count |
1
|
|
| SMILES |
Cl[H].O([H])[C@]([H])(C1C([H])=C([H])C([H])=C(C=1[H])O[H])C([H])([H])N([H])C([H])([H])[H]
|
|
| InChi Key |
OCYSGIYOVXAGKQ-FVGYRXGTSA-N
|
|
| InChi Code |
InChI=1S/C9H13NO2.ClH/c1-10-6-9(12)7-3-2-4-8(11)5-7;/h2-5,9-12H,6H2,1H3;1H/t9-;/m0./s1
|
|
| Chemical Name |
3-[(1R)-1-hydroxy-2-(methylamino)ethyl]phenol;hydrochloride
|
|
| Synonyms |
|
|
| HS Tariff Code |
2934.99.9001
|
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: Please store this product in a sealed and protected environment (e.g. under nitrogen), avoid exposure to moisture and light. |
|
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
|
|||
|---|---|---|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.08 mg/mL (10.21 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution.
For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 20.8 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.08 mg/mL (10.21 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 20.8 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. View More
Solubility in Formulation 3: ≥ 2.08 mg/mL (10.21 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 4.9099 mL | 24.5495 mL | 49.0990 mL | |
| 5 mM | 0.9820 mL | 4.9099 mL | 9.8198 mL | |
| 10 mM | 0.4910 mL | 2.4550 mL | 4.9099 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
| NCT Number | Recruitment | interventions | Conditions | Sponsor/Collaborators | Start Date | Phases |
| NCT01791816 | Active Recruiting |
Drug: Phenylephrine Drug: L-Ng-monomethyl Arginine (L-NMMA) |
Vasovagal Syncope Postural Tachycardia Syndrome |
New York Medical College | February 2013 | Early Phase 1 |
| NCT03620942 | Active Recruiting |
Drug: Phenylephrine Drug: Ephedrine |
Hypotension Anesthesia |
KK Women's and Children's Hospital |
November 7, 2018 | Not Applicable |
| NCT05011357 | Recruiting | Drug: Phenylephrine Drug: Saline Control |
Intraoperative Hypotension | University of Texas Southwestern Medical Center |
September 10, 2021 | Early Phase 1 |
| NCT02630121 | Recruiting | Drug: Oxymetazoline Hydrochloride Drug: Placebo |
Sleep Apnea Chronic Nasal Congestion |
University of South Florida | April 2023 | Phase 4 |
| NCT04602767 | Recruiting | Drug: Vasopressin Drug: Phenylephrine |
Acute Kidney Injury | Thomas Jefferson University | October 15, 2020 | Phase 4 |
|
|
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved





























 COA
COA