| Size | Price | Stock | Qty |
|---|---|---|---|
| 100mg |
|
||
| 250mg |
|
||
| 500mg |
|
||
| 1g |
|
||
| 2g |
|
||
| 5g | |||
| Other Sizes |
































Purity: ≥98%
Fluoxetine HCl (LY-110140; Lilly-110140; Prozac, Sarafem, Animex-On, Pulvules, Eufor, Portal), the HCl salt of fluoxetine, is a potent and selective serotonin-reuptake inhibitor (SSRI) at the neuronal membrane with anti-depressant activity. It can be used to treat premenstrual dysphoric disorder, bulimia nervosa, panic disorder, depression, and obsessive-compulsive disorder. In people 65 years of age and older, fluoxetine may reduce the risk of suicide. Premature ejaculation has also been treated with fluoxetine. It is consumed orally.
| Targets |
5-HT
Fluoxetine HCl (LY-110140) is a selective serotonin reuptake inhibitor (SSRI) that primarily targets the serotonin transporter (SERT). It exhibits a Ki of 0.8 nM for recombinant human SERT (using [³H]-paroxetine as the radioligand) [1] - For rat brain SERT, Fluoxetine HCl shows an IC50 of 2.1 nM in [³H]-5-HT uptake inhibition assays (rat cortical synaptosomes) [5] - It has weak affinity for 5-HT2C receptors (Ki = 350 nM, human recombinant) and no significant binding to dopamine transporters (DAT) or norepinephrine transporters (NET) at concentrations up to 1 μM [1,5] |
|---|---|
| ln Vitro |
In vitro activity: Fluoxetine inhibits the downregulation of cell proliferation brought on by the hippocampal cell's irreversible shock (IS).[1]
Fluoxetine increases the quantity of newborn cells in the dentate gyrus of the adult rat hippocampal hippocampus. Fluoxetine also boosts the quantity of proliferating cells in the prelimbic cortex.[2] Neurons in an immature state mature more quickly when taking fluoxetine. In the dentate gyrus, fluoxetine improves neurogenesis-dependent long-term potentiation (LTP).[3] Fluoxetine, but not citalopram, fluvoxamine, paroxetine and sertraline, increases norepinephrine and dopamine extracellular levels in prefrontal cortex. After acute systemic administration, fluoxetine causes strong and long-lasting increases in extracellular concentrations of dopamine and norepinephrine.[4] SERT-mediated 5-HT uptake inhibition in HEK293 cells: HEK293 cells transfected with human SERT were treated with Fluoxetine HCl (0.1–10 nM) for 30 minutes. At 1 nM, [³H]-5-HT uptake was inhibited by 78% compared to the vehicle control; the IC50 was 0.9 nM (liquid scintillation counting) [1] - BDNF upregulation in primary cortical neurons: Primary rat cortical neurons (7 days in vitro) treated with Fluoxetine HCl (1–10 μM) for 48 hours showed dose-dependent increases in BDNF protein levels. At 5 μM, BDNF expression increased by 2.4-fold (Western blot), and BDNF mRNA levels increased by 1.8-fold (qPCR) [3] - Neuroprotective effect against glutamate-induced toxicity: HT22 hippocampal cells pretreated with Fluoxetine HCl (0.5–5 μM) for 2 hours showed reduced cell death upon glutamate (5 mM) exposure. At 2 μM, the apoptotic rate decreased from 45% (vehicle) to 12% (Annexin V-FITC/PI staining), and caspase-3 activation was reduced by 60% (Western blot for cleaved caspase-3) [6] - Serotonin receptor-independent modulation of neurogenesis: Mouse neural stem cells (NSCs) treated with Fluoxetine HCl (0.1–1 μM) for 72 hours showed increased proliferation. At 0.5 μM, BrdU⁺ NSCs (proliferation marker) increased by 35% (immunofluorescence), and Nestin (NSC marker) expression remained unchanged [6] |
| ln Vivo |
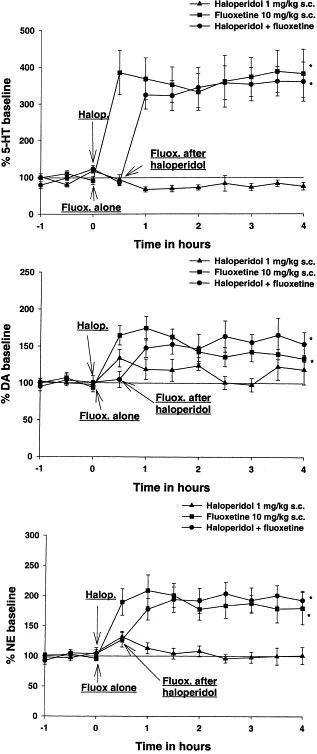
Fluoxetine treatment also reverses the deficit in escape latency seen in animals exposed to inescapable shock in adult male Sprague–Dawley rats.[1] Extracellular levels of norepinephrine ([NE](ex)) and dopamine ([DA](ex)) are robustly and sustainably increased by fluoxetine and olanzapine up to 361% and 272% of the baseline, respectively. These increases are significantly higher than those produced by either medication alone.[5]
Antidepressant-like effect in the rat forced swim test (FST): Male Sprague-Dawley rats (250–300 g) were orally administered Fluoxetine HCl (5, 10, 20 mg/kg/day) for 14 days. In the FST, 10 mg/kg/day Fluoxetine HCl reduced immobility time by 42% (from 180 seconds to 104 seconds) compared to the vehicle group, with no effect on swimming or climbing time [4] - Attenuation of social avoidance in the mouse social defeat model: C57BL/6 mice subjected to 10 days of social defeat were orally treated with Fluoxetine HCl (10 mg/kg/day) for 21 days. The social interaction ratio (time with stranger vs. empty cage) increased from 0.3 (vehicle) to 0.8 (Fluoxetine HCl-treated), and plasma corticosterone levels decreased by 38% (ELISA) [2] - Restoration of hippocampal volume in chronic stress rats: Male Wistar rats exposed to 21 days of chronic unpredictable stress (CUS) were orally given Fluoxetine HCl (15 mg/kg/day) for 28 days. MRI showed that hippocampal volume, which decreased by 12% in CUS rats, was restored to 98% of normal; hippocampal BDNF protein levels increased by 2.1-fold (Western blot) [3] - Anxiolytic effect in the mouse elevated plus maze (EPM): Female ICR mice (20–25 g) orally administered Fluoxetine HCl (5 mg/kg) 1 hour before the EPM test spent 35% more time in the open arms (from 18% to 24% of total time) compared to the vehicle group [5] |
| Enzyme Assay |
Recombinant Human SERT Binding Assay: The 200 μL reaction system contained 50 μg of human SERT-expressing HEK293 membrane protein, 0.5 nM [³H]-paroxetine (radioligand), and Fluoxetine HCl (0.01–10 nM). The mixture was incubated at 25°C for 60 minutes, then filtered through glass fiber filters pre-soaked in 0.3% polyethyleneimine. Filters were washed 3 times with cold 50 mM Tris-HCl (pH 7.4, containing 120 mM NaCl and 5 mM KCl), and radioactivity was measured using a liquid scintillation counter. Non-specific binding was determined in the presence of 10 μM imipramine, and Ki was calculated via the Cheng-Prusoff equation [1]
- Rat Brain Synaptosomal 5-HT Uptake Assay: Rat cortical synaptosomes (50 μg protein) were suspended in Krebs-Ringer-HEPES buffer (pH 7.4) containing 0.1 nM [³H]-5-HT and Fluoxetine HCl (0.1–10 nM). The reaction was incubated at 37°C for 10 minutes, then terminated by adding 2 mL of ice-cold buffer and filtering through glass fiber filters. Filters were washed twice, and radioactivity was quantified. Non-specific uptake was defined in the presence of 10 μM citalopram, and IC50 was derived from dose-response curves [5] |
| Cell Assay |
The membrane currents induced by serotonin (5-hydroxytryptamine; 5HT) were inhibited by micromolar concentrations of fluoxetine (Prozac) in Xenopusoocytes expressing either cloned 5HT2C receptors or 5HT receptors. The IC50 of fluoxetine was approximately 20 μM for responses elicited by 1 μM 5-HT. Moreover, [3H]5HT binding to 5HT receptors in rat cortex membranes and [3H]5HT binding to 5HT2C receptors expressed in HeLa cells were both inhibited by fluoxetine, with Ki values of ≈65–97 nM and ≈ 56 μM, respectively. The administration of fluoxetine prevented the inescapable shock (IS)-induced downregulation of hippocampal cell proliferation, which led to a behaviorally hopeless state. In rat adult hippocampal dentate gyrus, fluoxetine augmented the number of proliferating cells. The prelimbic cortex's proliferating cell count was also elevated by fluoxetine. Neutrophils matured more quickly when taking fluoxetine. LTP in the dentate gyrus was enhanced by fluoxetine in a neurogenesis-dependent manner. In prefrontal cortex, fluoxetine increased norepinephrine and dopamine extracellular levels, but not other selective serotonin uptake inhibitors like citalopram, fluvoxamine, paroxetine, and sertraline. Fluoxetine generated significant and long-lasting increases in dopamine and norepinephrine extracellular concentrations following acute systemic administration.
HEK293-SERT Cell [³H]-5-HT Uptake Assay: HEK293 cells stably expressing human SERT were seeded in 24-well plates at 2×10⁵ cells/well and cultured in DMEM with 10% FBS for 24 hours. Fluoxetine HCl (0.1–10 nM) was added, and cells were incubated for 30 minutes at 37°C. Medium was replaced with buffer containing 0.1 nM [³H]-5-HT, and incubation continued for 15 minutes. Cells were washed 3 times with cold buffer, lysed with 0.1 M NaOH, and radioactivity was measured. Uptake inhibition was calculated relative to the vehicle control [1] - Primary Cortical Neuron BDNF Western Blot: Primary cortical neurons were isolated from E18 rat embryos and cultured in neurobasal medium with B27 for 7 days. Fluoxetine HCl (1–10 μM) was added, and cells were incubated for 48 hours. Cells were lysed with RIPA buffer containing protease inhibitors, and 30 μg of protein was separated by 12% SDS-PAGE. Proteins were transferred to PVDF membranes, probed with anti-BDNF and anti-β-actin primary antibodies, and detected with HRP-conjugated secondary antibodies and ECL reagent. Band intensity was quantified via ImageJ [3] - HT22 Cell Apoptosis Assay: HT22 cells were seeded in 6-well plates at 1×10⁶ cells/well and cultured in DMEM with 10% FBS. Fluoxetine HCl (0.5–5 μM) was added 2 hours before glutamate (5 mM) treatment. After 24 hours, cells were harvested, stained with Annexin V-FITC and PI for 15 minutes at room temperature, and analyzed via flow cytometry. The apoptotic rate was calculated as the percentage of Annexin V-positive cells [6] - Neural Stem Cell Proliferation Assay: Mouse NSCs were isolated from the subventricular zone (SVZ) of P0 mice and cultured in NSC medium (DMEM/F12 + EGF + bFGF). Fluoxetine HCl (0.1–1 μM) was added, and cells were incubated for 72 hours. BrdU (10 μM) was added for the final 24 hours. Cells were fixed with 4% paraformaldehyde, stained with anti-BrdU (FITC-conjugated) and anti-Nestin (Cy3-conjugated) antibodies, and BrdU⁺Nestin⁺ cells were counted under a fluorescence microscope [6] |
| Animal Protocol |
Male Sprague-Dawley rats, weighing between 250 and 300 grams, are kept in housing with a 12-hour light/dark cycle (lights on at 7:00 am and lights off at 7:00 pm), constant humidity, and unrestricted access to food and water. For long-term medication therapy, rats receive intraperitoneal (IP) injections of fluoxetine (5 mg/kg/day) or saline, along with olanzapine or vehicle in their drinking water for 21 days (vehicle-treated control, fluoxetine, and olanzapine alone, as well as fluoxetine plus olanzapine). Olanzapine is the drug of choice for combination therapy because fluoxetine has the ability to disrupt olanzapine's metabolism and increase blood levels of the drug by up to 4-6 times. Olanzapine is dissolved in hydrochloric acid (HCl), and the stock solution with a concentration of 3 mg/mL is made by adjusting the pH back to 6 with 1 N sodium hydroxide. For the control animals, the same volume of vehicle solution is added to the water. Three times a week, the amount of fluid consumed is measured, and drinking bottles are refilled with pharmaceutical solution. The amount of fluid consumed by each treatment group is the same. The same dosage schedule applies to subchronic treatment, but the duration is extended to seven days.
Rat Forced Swim Test (FST): Male Sprague-Dawley rats (8–10 weeks old, 250–300 g) were housed under SPF conditions (22±2°C, 12-hour light/dark cycle). Rats were randomized into 4 groups (n=8/group): 1. Vehicle: Oral gavage of 0.5% carboxymethylcellulose sodium (CMC-Na, 10 mL/kg/day); 2. Fluoxetine 5 mg/kg: Oral gavage of Fluoxetine HCl (5 mg/kg/day, dissolved in 0.5% CMC-Na); 3. Fluoxetine 10 mg/kg: Oral gavage of Fluoxetine HCl (10 mg/kg/day, dissolved in 0.5% CMC-Na); 4. Fluoxetine 20 mg/kg: Oral gavage of Fluoxetine HCl (20 mg/kg/day, dissolved in 0.5% CMC-Na). Treatment lasted 14 days. On day 15, rats were placed in a cylindrical tank (50 cm tall, 20 cm diameter, 25°C water) for 6 minutes. Immobility time (floating without active movement) was recorded during the final 4 minutes [4] - Mouse Social Defeat Model: Male C57BL/6 mice (6–8 weeks old, 20–25 g) were subjected to 10 days of social defeat (5 minutes of physical interaction with an aggressive CD1 mouse, followed by 24 hours of sensory contact). Mice were then randomized into 2 groups (n=10/group): 1. Vehicle: Oral gavage of 0.5% CMC-Na (10 mL/kg/day); 2. Fluoxetine: Oral gavage of Fluoxetine HCl (10 mg/kg/day, dissolved in 0.5% CMC-Na). Treatment lasted 21 days. On day 32, social interaction was tested: mice were placed in a 3-chamber arena, and time spent in the chamber with a stranger CD1 mouse (vs. empty chamber) was recorded for 10 minutes [2] - Rat Chronic Unpredictable Stress (CUS) Model: Male Wistar rats (8 weeks old, 220–250 g) were exposed to CUS for 21 days (random stressors: food/water deprivation, cage tilt, cold water swim). Rats were then randomized into 2 groups (n=6/group): 1. CUS+Vehicle: Oral gavage of 0.5% CMC-Na (10 mL/kg/day); 2. CUS+Fluoxetine: Oral gavage of Fluoxetine HCl (15 mg/kg/day, dissolved in 0.5% CMC-Na). Treatment lasted 28 days. On day 50, rats were anesthetized with isoflurane for MRI (hippocampal volume measurement). Rats were then euthanized, and hippocampi were dissected for BDNF Western blot [3] |
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion
Fluoxetine hydrochloride appears to be well absorbed from the gastrointestinal tract after oral administration. The oral bioavailability of fluoxetine in humans has not been fully elucidated to date, but at least 60-80% of the oral dose appears to be absorbed. However, it is unclear how much of the oral dose enters the systemic circulation unchanged. Limited animal data suggest that the drug may undergo first-pass metabolism and clearance in the liver and/or lungs after oral administration. In these animals (beagles), approximately 72% of the oral dose entered the systemic circulation unchanged. Food appears to slightly decrease the rate of fluoxetine absorption in humans, but does not affect the extent of absorption. The distribution of fluoxetine and its metabolites in human tissues and fluids has not been fully elucidated. Limited pharmacokinetic data from long-term animal administration of fluoxetine suggest that the drug and some of its metabolites (including norfluoxetine) are widely distributed throughout the body, with the highest concentrations in the lungs and liver. The drug can cross the blood-brain barrier in humans and animals. Reports indicate that in animals, the ratios of fluoxetine to norfluoxetine in the cerebral cortex, striatum, hippocampus, hypothalamus, brainstem, and cerebellum were similar one hour after a single dose. To confirm embryonic/fetal exposure to fluoxetine and/or its metabolites, researchers used dissection and whole-body autoradiography to determine placental transport and fetal distribution in Wistar rats at days 12 and 18 of gestation at 1, 4, 8, and 24 hours after a single oral dose of 12.5 mg/kg of 14C fluoxetine. On days 12 (organogenesis) and 18 (late organogenesis), radiocarbon concentrations in the placenta, embryo/fetus, amniotic fluid, and maternal kidneys, brain, and lungs peaked 4–8 hours after administration, decreasing slightly at 24 hours. At all time points, the highest tissue radiocarbon concentration was observed in the maternal lungs. Moderate radioactivity levels were observed in the placenta and maternal brain, kidneys, and liver, while lower levels were observed in embryonic/fetal tissues, amniotic fluid, and maternal plasma. The mean radiocarbon concentration in the fetus at 4, 8, and 24 hours of day 18 gestation was higher than that in the embryo at day 12 gestation. Radioactive analysis showed that the total concentration of fluoxetine and norfluoxetine accounted for 63-80% of the total radiocarbon concentration in embryonic/fetal tissues. The results indicated that the concentration of fluoxetine in embryonic/fetal and maternal tissues reached its peak in early gestation and decreased over time; while the tissue concentration of norfluoxetine reached its peak at 24 hours. Whole-body autoradiography showed that radioactive substances associated with fluoxetine (14C) and its metabolites crossed the placenta and distributed in the 18-day-old fetus within 4 hours of administration. Visual and quantitative analysis of the autoradiograms showed that the highest concentrations of radiocarbon in the fetus were found in the brain and thymus. These results demonstrate that fluoxetine and norfluoxetine can cross the placenta and distribute in the embryonic/fetal body during and after organogenesis, confirming the effects of maternal drugs and their metabolites on the embryonic/fetal that were not observed in previous rat teratogenicity and reproduction studies. Elimination: Kidneys: 80% excreted in urine (11.6% fluoxetine, 7.4% fluoxetine glucoside, 6.8% norfluoxetine, 8.2% norfluoxetine glucoside, >20% hippuric acid, 46% other metabolites); Bile: Approximately 15% excreted in feces; Dialysis-prone – due to high protein binding and large volume of distribution. For more complete data on the absorption, distribution, and excretion of fluoxetine hydrochloride (6 types), please visit the HSDB record page. Metabolism/Metabolites: This study aimed to clarify the N-demethylation kinetics of fluoxetine in human liver microsomes and to identify cytochrome P450 (CYP) isoenzymes involved in this metabolic pathway. We determined the kinetics of norfluoxetine (Ne) formation in human liver microsomes from 6 genotype CYP2C19 extensive metabolizers (EM). We investigated the correlation between fluoxetine N-demethylase activity and the activities of various CYP enzymes. Furthermore, we used selective inhibitors or chemical probes of various cytochrome P-450 isoenzymes. In all liver microsomes, the kinetics of norfluoxetine formation followed the single-enzyme Michaelis equation (mean Km = 32 μmol/L ± 7 μmol/L). At concentrations of 25 μmol/L and 100 μmol/L, there was a significant correlation between N-demethylation of fluoxetine and 3-hydroxylation of tolbutamide at 250 μmol/L (r1 = 0.821, P1 = 0.001; r2 = 0.668, P2 = 0.013), and at a high substrate concentration of 100 μmol/L, there was also a significant correlation between N-demethylation of fluoxetine and S-metphenytoin 4'-hydroxylase activity (r = 0.717, P = 0.006). High concentrations of S-metphenytoin (SMP) (a CYP2C19 substrate) and sulfamethoxazole (SUL) (a selective CYP2C9 inhibitor) significantly inhibited the formation of norfluoxetine. Co-incubation with the chemical probe CYP3A4 inhibitor (triacetylpyridinium oxaliplatin, TAO) showed minimal inhibitory effect on this reaction. When microsomes were pre-incubated with SUL and TAO, the inhibition rate of fluoxetine N-demethylation in PM liver was higher than that in EM liver at high substrate concentrations (100 μmol/L) than in EM liver (73% vs 45%, P < 0.01). At near-therapeutic substrate concentrations, cytochrome P450 CYP2C9 is likely the major CYP isoenzyme catalyzing fluoxetine N-demethylation in human liver microsomes, and polymorphic CYP2C19 may play a more significant role in this metabolic pathway at high substrate concentrations. The exact metabolic pathway of fluoxetine has not been fully elucidated. The drug appears to be extensively metabolized in the liver to norfluoxetine and several other metabolites. Norfluoxetine (desmethylfluoxetine) is the major metabolite, formed by the N-demethylation of fluoxetine, a process likely controlled by multiple genes. The potency and selectivity of norfluoxetine in inhibiting serotonin reuptake appear similar to the parent drug. Both fluoxetine and norfluoxetine are bound to glucuronic acid in the liver, and limited animal evidence suggests that both the parent drug and its major metabolite undergo O-dealkylation to produce p-trifluoromethylphenol, which subsequently appears to be metabolized to hippuric acid. Biological Half-Life It has been reported that the half-life of fluoxetine is prolonged after multiple doses compared to a single dose (approximately 4–5 days), suggesting a non-linear pattern of drug accumulation during long-term administration. According to reports, after a single oral dose of fluoxetine in healthy adults, the average elimination half-life of fluoxetine is approximately 2-3 days (range: 1-9 days), and the average elimination half-life of norfluoxetine is approximately 7-9 days (range: 3-15 days). For patients with cirrhosis, the average half-life of fluoxetine is 6.6 days, while the half-life in healthy patients is 2.2 days. Normal volunteers. Oral bioavailability: In male Sprague-Dawley rats, the oral bioavailability of fluoxetine hydrochloride (10 mg/kg) was 72%, while that of intravenous (5 mg/kg) was 72% [1] -Plasma pharmacokinetics: In rats that received intravenous fluoxetine hydrochloride (5 mg/kg), the Cmax was 1.8 μg/mL, the Tmax was 5 minutes, and the elimination half-life (t1/2) was 16 hours. After oral administration (10 mg/kg), Cmax was 0.9 μg/mL, Tmax was 6 hours, and t1/2 was 18 hours [1] - Tissue distribution: Two hours after oral administration of fluoxetine hydrochloride (10 mg/kg) to mice, the brain/plasma concentration ratio was 0.9, and the highest drug accumulation was observed in the liver and kidneys (fluoxetine in tissue homogenates was detected by high performance liquid chromatography) [2] - Plasma protein binding rate: The protein binding rate of fluoxetine hydrochloride in human plasma was 94% (ultrafiltration method, plasma concentration range: 0.1–10 μg/mL) [1] |
| Toxicity/Toxicokinetics |
Effects During Pregnancy and Lactation
◉ Overview of Lactation Use Compared to most other selective serotonin reuptake inhibitors (SSRIs), fluoxetine has a higher average drug concentration in breast milk. Its long-acting active metabolite, norfluoxetine, is detectable in the serum of most breastfed infants during the first two months postpartum, and subsequently in a minority of infants. Some breastfed infants have reported adverse reactions such as colic, irritability, and lethargy. One study found reduced infant weight gain, but other studies have not found this. A small number of infants were followed for up to one year without any adverse effects on development. If the mother needs to take fluoxetine, breastfeeding should not be discontinued. One safety rating system considers the use of fluoxetine during lactation to be feasible, but other rating systems do not recommend it. If the mother took fluoxetine during pregnancy, or other antidepressants were ineffective, most experts recommend not changing medications during lactation. Otherwise, medications with lower milk production should be preferred, especially when breastfeeding newborns or premature infants. Behavioral side effects in breastfed infants, such as colic, restlessness, irritability, feeding difficulties, and poor weight gain, should be monitored. Mothers who took selective serotonin reuptake inhibitors (SSRIs) during pregnancy and postpartum may find breastfeeding more difficult, but this may reflect their medical condition. These mothers may require additional breastfeeding support. Breastfed infants exposed to SSRIs in late pregnancy have a lower risk of neonatal maladaptive disorder than formula-fed infants. ◉ Effects on Breastfed Infants A 6-day-old breastfed infant experienced colic, reduced sleep, vomiting, and watery stools, possibly caused by the mother's fluoxetine use. Two other cases of colic in breastfed infants, one 1.76 months old and the other 2 months old, have been reported, possibly related to fluoxetine in breast milk. The older infant also exhibited hyperactivity. Another 3-month-old infant may have presented with irritability, observed by the infant's father (a pediatrician). However, the infant's mother and pediatrician disagreed on this. The Australian Adverse Drug Reaction Advisory Committee received a report of a 5-month-old infant developing hyperglycemia and glycosuria, possibly linked to fluoxetine in breast milk. A 3-day-old breastfed infant was difficult to wake, stopped rooting, reduced feeding frequency, and exhibited groaning and whimpering. Despite prior exposure to fluoxetine in utero and slight lethargy in the first two days after birth, the infant's symptoms worsened after the mother began producing milk on the third day. These effects were likely caused by fluoxetine in breast milk. A 3-week-old breastfed infant presented with suspected drug-induced epileptic-like activity and cyanosis; the mother had taken fluoxetine, carbamazepine, and buspirone during pregnancy and lactation. An observational study of four infants found no significant neurological abnormalities 12 to 52 weeks after exposure to fluoxetine in breast milk. A retrospective case-control cohort study compared the weight of infants born to mothers who took fluoxetine during pregnancy and breastfed for at least two weeks postpartum with that of infants born to mothers who took fluoxetine during pregnancy but did not breastfeed. Compared to the control group, the 26 infants who received fluoxetine through breast milk experienced a decrease in weight gain, but remained within the normal range. A prospective study included 51 breastfeeding women who took fluoxetine and 63 breastfeeding women who did not take fluoxetine. The results showed that fluoxetine had no effect on infant weight gain, but infants born to mothers who took fluoxetine experienced a higher frequency of undefined side effects. This study was published only as an abstract and therefore lacks some details. In a prospective study, 21 of 40 women who took fluoxetine throughout pregnancy breastfed (the extent and duration of breastfeeding were not specified). Tests on infants aged 15 to 71 months revealed no differences in cognition, language, or temperament between breastfed and non-breastfed infants. A study compared infants born to 31 mothers with major depressive disorder who received selective serotonin reuptake inhibitors (SSRIs) during pregnancy with 13 infants born to mothers with depression who did not receive SSRIs. The results showed that both groups of infants had normal psychological and most motor development during a mean follow-up period of 12.9 months. Three of the treated mothers received an average daily dose of fluoxetine 23.3 mg for 3 months while breastfeeding. These infants showed slightly delayed psychomotor development compared to the control group, but the impact of breastfeeding on developmental abnormalities could not be determined. Researchers measured platelet serotonin levels in 11 mothers and their breastfed infants after 4 to 12 weeks of fluoxetine treatment. Since platelets and neurons share the same serotonin transporter, the effect of fluoxetine on platelet serotonin may predict its potential effects on the nervous system of some breastfed infants. The mothers received daily doses of fluoxetine ranging from 20 to 40 mg. At the start of treatment, 10 infants were under 6 months old, and 4 were under 3 months old; 6 of these infants were exclusively breastfed. Although fluoxetine treatment reduced maternal platelet serotonin levels from 157 μg/L to 23 μg/L, the infants' mean serotonin levels were 217 μg/L before treatment and 230 μg/L after treatment. These results indicate that the dose of fluoxetine ingested by the infants was insufficient to affect serotonin transport in platelets in most breastfed infants. However, three infants experienced a decrease in platelet serotonin levels of 13%, 24%, and 60%, respectively. This last infant was the only one in whom both fluoxetine and norfluoxetine levels were measurable in plasma, but this infant did not experience significant adverse reactions. Another infant had delayed motor development at 24 weeks but normal intellectual development; six other infants were tested between 24 and 56 weeks of age, and both indicators were within one standard deviation of normal. Twenty-nine mothers started taking fluoxetine (average 34.6 mg daily) within four weeks postpartum to treat depression or anxiety. They exclusively breastfed their infants for four months, and breastfed at least 50% of their babies in the fifth and sixth months. These infants' weight gain at six months met national growth standards, and the mothers did not report any abnormalities in their infants. A study on the side effects of selective serotonin reuptake inhibitors (SSRIs) in breastfeeding mothers found that infants born to mothers taking fluoxetine did not experience any adverse events requiring medical attention. Specific information regarding maternal fluoxetine dosage, breastfeeding extent, or infant age was not reported. Eleven infants were breastfed (the extent and duration of breastfeeding were not specified) while their mothers were taking fluoxetine for depression (n=5) or panic disorder (n=6). These infants had normal weight gain at 12 months of age, with no significant difference compared to a control group whose mothers were not taking psychiatric medication. These infants also had normal neurodevelopment at 12 months of age. One 11-week-old infant was breastfed (feeding extent unspecified) while the mother took 20 mg of fluoxetine daily. No adverse clinical events were observed during the study. A small study compared pain responses in infants born to mothers with depression who took a selective serotonin reuptake inhibitor (SSRI) alone or both during pregnancy and lactation with those born to mothers without SSRI exposure. Infants exposed only to an SSRI prenatally or who received an SSRI through breast milk prenatally and postnatally had a dulled pain response compared to the control group. Seven out of 30 infants were exposed to fluoxetine. The influence of maternal behavior due to depression could not be ruled out because mothers without depression but not taking medication served as the control group. The authors emphasize that these findings do not imply that antidepressant medications should be avoided during pregnancy or that breastfeeding should be avoided during SSRI treatment. One infant's mother took 40 mg of fluoxetine, 20 mg of oxycodone (three times daily), and quetiapine 400 mg daily. The infant was breastfed 6 to 7 times daily and received oral morphine 120 mcg (3 times daily) three times daily due to opioid withdrawal symptoms. At 3 months of age, the infant's weight was found to be in the 25th percentile for its age, compared to the 50th percentile at birth. The authors attributed the weight loss to opioid withdrawal symptoms. The infant's Denver Developmental Score was age-appropriate. A non-controlled online survey collected data from 930 breastfeeding mothers taking antidepressants. Approximately 10% of the infants reported withdrawal symptoms (e.g., irritability, hypothermia, uncontrollable crying, eating and sleeping disturbances). Mothers taking antidepressants only during breastfeeding were less likely to notice withdrawal symptoms in their infants than mothers who took the medication during both pregnancy and breastfeeding. A cohort study of 247 infants exposed to antidepressants in utero during late pregnancy assessed neonatal maladaptive disorder (PNA). Of these 247 infants, 154 had PNA. The risk of PNA in exclusively formula-fed infants is approximately three times that of exclusively or partially breastfed infants. Fifteen infants were exposed to fluoxetine in utero. One mother of a late preterm infant received 60 mg of fluoxetine daily throughout pregnancy and during exclusive breastfeeding. Seven days after birth, the infant presented with seizures, increased muscle tone, hyperreflexia, tachypnea, and compensatory metabolic acidosis. The infant's Fennegan score ranged from 7 to 10. By day 8, the infant's serum fluoxetine concentration was 120 μg/L, similar to therapeutic concentrations in adults. After cessation of breastfeeding and five days of formula feeding, the infant's Fennegan score decreased to 3 to 6. Most symptoms resolved after 10 days of formula feeding. At 3 months of age, the infant's growth and development were normal. The infant's symptoms were considered to be serotonin syndrome caused by high concentrations of fluoxetine, rather than a withdrawal reaction. This reaction may be caused by fluoxetine, and breastfeeding may lead to a sustained high level of fluoxetine in the blood postpartum. A woman with narcolepsy took 4 grams of sodium oxybutyrate at 10 p.m. and 2 a.m. daily throughout her pregnancy and postpartum, along with 20 mg of fluoxetine and 5 mg of cetirizine daily. She was exclusively breastfed except for four hours after each sodium oxybutyrate dose at 10 p.m. and 2 a.m. She expressed breast milk or breastfed directly before each sodium oxybutyrate dose. The infant was exclusively breastfed or breast-only for the first 6 months before the introduction of complementary foods. The infant was assessed using the Ages and Stages Questionnaires at 2, 4, and 6 months of age, with results within the normal range. The infant's growth and development, as well as the pediatrician's clinical impression of the infant's growth and development, were also within the normal range. Two women took 20 mg of fluoxetine daily during late pregnancy and lactation. Pediatric evaluations, including neurological assessments and brain ultrasound, were performed within 24 hours postpartum. Further follow-up was conducted when the infant was 6 months of age or older. The infant's clinical condition was comparable to that of other infants in the same pediatric ward who had not been exposed to fluoxetine. A woman was taking 40 mg of fluoxetine daily during pregnancy and postpartum for depression. She breastfed the infant (the extent of breastfeeding was not specified). Umbilical vein blood gas analysis at delivery showed a pH of 7.38. Forty-five minutes postpartum, the infant developed respiratory distress syndrome with mixed respiratory and metabolic acidosis, cyanosis, and hypotonia, requiring admission to the neonatal intensive care unit. Blood glucose on admission was 3.4 mmol/L. The infant initially exhibited abnormal movements, tremors, and stretching postures, which subsided within hours, followed by irritability and poor sleep quality. The infant's symptoms improved after the mother stopped breastfeeding, but blood levels of fluoxetine and norfluoxetine remained low. The infant was discharged 16 days after birth. The authors believe the infant's symptoms were due to fluoxetine-induced serotonin syndrome. ◉ Effects on Lactation and Breast Milk Fluoxetine can cause elevated prolactin levels and galactorrhea in non-pregnant, non-lactating patients. There are also reports of fluoxetine causing normoprolactinemia-related galactorrhea. In a study of cases of hyperprolactinemia and its symptoms (such as gynecomastia) reported by the French Pharmacovigilance Center, fluoxetine was found to cause a 3.6 times higher risk of hyperprolactinemia than other drugs. Preliminary animal and in vitro studies have suggested that fluoxetine may have some estrogenic activity. For mothers who have established lactation, prolactin levels may not affect their ability to breastfeed. In a small prospective study, researchers compared eight primiparous women taking serotonin reuptake inhibitors (SRIs; three took fluoxetine, and the remaining one took citalopram, duloxetine, escitalopram, paroxetine, or sertraline, respectively) with 423 mothers who did not take SRIs. Mothers taking selective serotonin reuptake inhibitors (SSRIs) experienced a mean delay of 16.7 hours initiation of lactation activation (stage II) compared to the control group (85.8 hours postpartum in the SSRI treatment group vs. 69.1 hours postpartum in the untreated group), which doubled the risk of delayed feeding behavior. However, the delay in stage II lactation may not be clinically significant, as there was no statistically significant difference between the two groups in the proportion of mothers experiencing feeding difficulties after day 4 postpartum. A case-control study compared the proportion of mothers primarily breastfeeding at 2 weeks postpartum in those who took SSRIs throughout pregnancy and delivery (n = 167), those who took SSRIs only during pregnancy (n = 117), and control mothers who did not take antidepressants (n = 182). In two groups of participants who took selective serotonin reuptake inhibitors (SSRIs), 33 took citalopram, 18 took escitalopram, 63 took fluoxetine, 2 took fluvoxamine, 78 took paroxetine, and 87 took sertraline. Among women taking SSRIs, the breastfeeding rate at two weeks postpartum was 27% to 33% lower than that of mothers not taking antidepressants, but there was no statistically significant difference in breastfeeding rates between the SSRI exposure groups. An observational study investigated the outcomes of 2,859 women who had taken antidepressants in the two years prior to pregnancy. Compared to women who did not take antidepressants during pregnancy, mothers who took antidepressants in all three stages of pregnancy were 37% less likely to breastfeed at discharge. Mothers who took antidepressants only in the third trimester were 75% less likely to breastfeed at discharge. Mothers who took antidepressants only in the first and second trimesters were not less likely to breastfeed at discharge. However, the study did not specify the type of antidepressant used by the mothers. A retrospective cohort study analyzed hospital electronic medical records from 2001 to 2008, comparing women taking antidepressants in late pregnancy (n = 575; of whom n = 21 took fluoxetine), women with mental illness but not taking antidepressants (n = 1552), and mothers not diagnosed with mental illness (n = 30,535). Women receiving antidepressant treatment were 37% less likely to breastfeed at discharge than women not diagnosed with mental illness, but there was no difference in the likelihood of breastfeeding compared to untreated mothers diagnosed with mental illness. A study of 80,882 Norwegian mother-infant pairs from 1999 to 2008 showed that 392 women reported starting antidepressants postpartum, and 201 women reported starting antidepressants during pregnancy. Compared to a control group not exposed to antidepressants, taking antidepressants in late pregnancy was associated with a 7% lower likelihood of initiating breastfeeding, but had no effect on the duration of breastfeeding or the rate of exclusive breastfeeding. Compared with the control group who had not been exposed to antidepressants, new use or restart of antidepressants was associated with a 63% lower likelihood of primary breastfeeding at 6 months, a 51% lower likelihood of any breastfeeding, and a 2.6-fold increased risk of abrupt cessation of breastfeeding. No specific antidepressant was mentioned. # Toxicity/Toxicokinetics - Acute in vivo toxicity: The LD50 of fluoxetine hydrochloride in male ICR mice (intraperitoneal injection) was 240 mg/kg. Mice given doses >180 mg/kg showed signs of convulsions and respiratory depression and died within 24 hours.[5] - Subacute toxicity: Rats were given fluoxetine hydrochloride (10, 20, 40 mg/kg/day) orally for 28 days. No significant changes were observed in body weight (change <5%) or serum ALT/AST/BUN/creatinine levels. Pathological examination of liver, kidney and brain tissues revealed no tissue damage [1] - Drug interaction: Concomitant oral administration of fluoxetine hydrochloride (10 mg/kg/day) and diazepam (2 mg/kg/day) to rats for 14 days resulted in a 25% increase in diazepam plasma concentration, but no enhancement of sedative effect (rotarod test) [2] |
| References | |
| Additional Infomation |
N-Methyl-3-phenyl-3-[4-(trifluoromethyl)phenoxy]-1-propylamine hydrochloride (1:1) is the hydrochloride salt of N-methyl-3-phenyl-3-[4-(trifluoromethyl)phenoxy]propyl-1-amine. Fluoxetine hydrochloride is the hydrochloride form of fluoxetine, a diphenhydramine derivative and a selective serotonin reuptake inhibitor with antidepressant, anti-anxiety, anti-obsessive-compulsive, and anti-bulimia activities, and potential immunomodulatory activity. After administration, fluoxetine binds to presynaptic serotonin (5-HT) receptors, leading to negative allosteric regulation of the receptor complex, thereby blocking the reuptake of serotonin by the presynaptic receptors. Fluoxetine enhances serotonergic function by inhibiting serotonin reuptake, causing serotonin to accumulate in the synaptic cleft, leading to long-term desensitization and downregulation of 5-HT receptors, blocking 5-HT-mediated signal transduction, and thus producing antidepressant, anti-anxiety, anti-obsessive-compulsive, and anti-bulimia effects. In addition, fluoxetine may inhibit the expression of pro-inflammatory cytokines, including interleukin-6 (IL-6), thereby preventing IL-6-mediated inflammation and cytokine storms. It is the first highly specific serotonin reuptake inhibitor. It is used as an antidepressant and is generally more tolerable than conventional antidepressants due to its side effects. See also: fluoxetine (active ingredient); fluoxetine hydrochloride; olanzapine (ingredient). Mechanism of Action: The antidepressant mechanism of fluoxetine is not fully understood, but it has been shown to selectively inhibit the reuptake of serotonin (5-HT) on the presynaptic neuronal membrane. Fluoxetine-induced inhibition of serotonin reuptake leads to increased serotonin concentration in the synaptic cleft of the central nervous system, resulting in various functional changes associated with enhanced serotonergic neurotransmission. Monoamine oxidase B has been identified as the enzyme that converts 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine into its toxic metabolite, 1-methyl-4-phenylpyridine ions. Since this enzyme is primarily located in astrocytes and serotonergic neurons, 1-methyl-4-phenylpyridine ions appear to be generated outside of dopaminergic neurons. To verify this possibility, we administered fluoxetine systemically before administering 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine. Consistent with fluoxetine's proven ability to inhibit the uptake of 1-methyl-4-phenylpyridine by serotonergic neurons and serotonin by astrocytes, fluoxetine pretreatment significantly attenuated the striatal dopamine and serotonin decreases induced by 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine. These results support the generation of 1-methyl-4-phenylpyridine ions outside the dopaminergic system. Fluoxetine is a potent and selective inhibitor of neuronal serotonin uptake carriers and a clinically effective antidepressant. Although fluoxetine is usually used clinically in its racemic form, its interaction with serotonin uptake carriers appears to exhibit weak but verifiable stereoselectivity. This study aimed to determine the absolute configuration of the enantiomers of fluoxetine and to examine whether the effects of fluoxetine in behavioral tests are enantiomer-specific. (S)-Fluoroxetine is synthesized by reacting (S)-(-)-3-chloro-1-phenylpropanol sequentially with sodium iodide, methylamine, sodium hydride, and 4-fluorobenzene trifluoride. (S)-Fluoroxetine is dextrorotatory in methanol (optical rotation +1.60) and levorotatory in water (optical rotation -10.85). The enantiomers of fluoxetine were derivatized with (R)-1-(1-naphthyl)ethyl isocyanate, and the resulting urea compounds were determined by 1H NMR or HPLC to determine the optical purity of the fluoxetine samples. Both enantiomers antagonized the writhing response in mice; the ED50 values of (R)- and (S)-fluoxetine after subcutaneous injection were 15.3 and 25.7 mg/kg, respectively. Furthermore, both enantiomers enhanced the analgesic effect of a subthreshold analgesic dose (0.25 mg/kg) of morphine, with ED50 values of 3.6 and 5.7 mg/kg, respectively. After intraperitoneal injection in mice, both stereoisomers antagonized the decrease in whole-brain serotonin concentration induced by chloramphenicol. The ED50 values of (S)- and (R)-fluoxetine were 1.2 and 2.1 mg/kg, respectively. Intraperitoneal injection into rats reduced palatability-induced food intake in both enantiomers; (R)- and (S)-fluoxetine reduced saccharin-induced water intake, with ED50 values of 6.1 and 4.9 mg/kg, respectively. Therefore, all biochemical and pharmacological studies to date have shown that the superiority ratio of fluoxetine enantiomers is close to 1. Mechanism of Action: Fluoxetine hydrochloride (LY-110140) exerts its antidepressant effect by selectively inhibiting SERT, which blocks the reuptake of serotonin by presynaptic neurons, thereby increasing extracellular serotonin levels in the brain. It also regulates neurotrophic factors (e.g., BDNF) and neurogenesis in the hippocampus, resulting in long-term therapeutic effects [1,3,6]. Therapeutic Potential: Fluoxetine hydrochloride has been clinically approved for the treatment of major depressive disorder (MDD), obsessive-compulsive disorder (OCD), panic disorder, and social anxiety disorder. Preclinical models (e.g., forced swimming test, social frustration model) have confirmed its antidepressant and anti-anxiety efficacy [2,4]
- Chemical properties:Fluoxetine hydrochloride (LY-110140) is soluble in water (10 mg/mL) and dimethyl sulfoxide (DMSO) (50 mg/mL). It is stable for 7 days in aqueous solution at pH 4.0–8.0 at room temperature [1] - Safety notes: Literature [2] indicates thatfluoxetine hydrochloride may increase the plasma concentration of drugs metabolized by CYP2D6 (e.g., diazepam), and therefore dosage adjustment is required in clinical practice. [2] |
| Molecular Formula |
C17H19CLF3NO
|
|
|---|---|---|
| Molecular Weight |
345.79
|
|
| Exact Mass |
345.11
|
|
| Elemental Analysis |
C, 59.05; H, 5.54; Cl, 10.25; F, 16.48; N, 4.05; O, 4.63
|
|
| CAS # |
56296-78-7
|
|
| Related CAS # |
Fluoxetine; 54910-89-3; (S)-Fluoxetine hydrochloride; 114247-06-2; (R)-Fluoxetine hydrochloride; 114247-09-5
|
|
| PubChem CID |
62857
|
|
| Appearance |
White to off-white solid powder
|
|
| Boiling Point |
395.1ºC at 760mmHg
|
|
| Melting Point |
158-159°C
|
|
| Flash Point |
192.8ºC
|
|
| LogP |
5.627
|
|
| Hydrogen Bond Donor Count |
2
|
|
| Hydrogen Bond Acceptor Count |
5
|
|
| Rotatable Bond Count |
6
|
|
| Heavy Atom Count |
23
|
|
| Complexity |
308
|
|
| Defined Atom Stereocenter Count |
0
|
|
| SMILES |
Cl[H].FC(C1C([H])=C([H])C(=C([H])C=1[H])OC([H])(C1C([H])=C([H])C([H])=C([H])C=1[H])C([H])([H])C([H])([H])N([H])C([H])([H])[H])(F)F
|
|
| InChi Key |
GIYXAJPCNFJEHY-UHFFFAOYSA-N
|
|
| InChi Code |
InChI=1S/C17H18F3NO.ClH/c1-21-12-11-16(13-5-3-2-4-6-13)22-15-9-7-14(8-10-15)17(18,19)20;/h2-10,16,21H,11-12H2,1H3;1H
|
|
| Chemical Name |
N-methyl-3-phenyl-3-[4-(trifluoromethyl)phenoxy]propan-1-amine;hydrochloride
|
|
| Synonyms |
|
|
| HS Tariff Code |
2922.39.4500
|
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: Please store this product in a sealed and protected environment (e.g. under nitrogen), avoid exposure to moisture and light. |
|
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
|
|||
|---|---|---|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.5 mg/mL (7.23 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution.
For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.5 mg/mL (7.23 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. View More
Solubility in Formulation 3: ≥ 2.5 mg/mL (7.23 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. Solubility in Formulation 4: 13 mg/mL (37.60 mM) in PBS (add these co-solvents sequentially from left to right, and one by one), clear solution; with ultrasonication. |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 2.8919 mL | 14.4596 mL | 28.9193 mL | |
| 5 mM | 0.5784 mL | 2.8919 mL | 5.7839 mL | |
| 10 mM | 0.2892 mL | 1.4460 mL | 2.8919 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
| NCT Number | Recruitment | interventions | Conditions | Sponsor/Collaborators | Start Date | Phases |
| NCT03826875 | Recruiting | Drug: Fluoxetine Drug: Placebo |
Stroke Hemorrhagic Depression |
University of Washington | March 1, 2019 | Phase 2 |
| NCT05634707 | Recruiting | Drug: Fluoxetine Drug: Temozolomide |
Primary Brain Tumor Brain Tumor, Recurrent |
Duke University | August 5, 2023 | Early Phase 1 |
| NCT03228732 | Recruiting | Drug: Fluoxetine Drug: Fluoxetine and DHEA |
Type 1 Diabetes Mellitus | University of Maryland, Baltimore |
December 19, 2017 | Early Phase 1 |
| NCT05976347 | Not yet recruiting | Drug: Fluoxetine 20 MG Drug: Duloxetine 30 MG/td> | Depression | Wake Forest University Health Sciences |
February 2024 | Phase 4 |
| NCT06225011 | Not yet recruiting | Drug: Fluoxetine | Colorectal Adenocarcinoma | Jonsson Comprehensive Cancer Center |
June 1, 2024 | Phase 1 |
|
|
|
|
|
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved





























 COA
COA