| Size | Price | Stock | Qty |
|---|---|---|---|
| 5mg |
|
||
| 10mg |
|
||
| 25mg |
|
||
| 50mg |
|
||
| 100mg |
|
||
| 250mg |
|
||
| 500mg |
|
||
| Other Sizes |
































Purity: ≥98%
Reboxetine (also known as PNU 155950E; Trade name: Edronax)is a selective norepinephrine reuptake inhibitor with Ki of 8.2 nM and antidepressant activity. Reboxetine completely and dose-dependently blocks [3H]-dopamine uptake to the human norepinephrine transporters (hNET) in Madin-Darby canine kidney (MDCK) cells, with a Ki value of 11 nM. With an ED50 of 191 μg/kg, reboxetine potently and dose-dependently inhibits the firing of locus coeruleus neurons in rats. The α2 antagonist piperoxan (1.5 mg/kg, IV) can reverse the effects of reboxetine-induced inhibition of locus coeruleus neurons. The mice's blepharospasm and hypothermia caused by reserpine are reversed by reboxetine in a dose-dependent manner.
| Targets |
norepinephrine reuptake ( Ki = 8.2 nM )
Reboxetine mesylate targets human norepinephrine transporter (NET) with a Ki value of 1.8 nM (radioligand binding assay) and an IC₅₀ value of 2.4 nM (norepinephrine uptake inhibition assay in HEK293-NET cells) [5] Reboxetine mesylate shows high selectivity for NET over serotonin transporter (SERT) and dopamine transporter (DAT): Ki = 1200 nM (SERT), Ki > 10,000 nM (DAT) [5] |
|---|---|
| ln Vitro |
In vitro activity: Reboxetine completely and dose-dependently blocks [3H]-dopamine uptake to the human norepinephrine transporters (hNET) in Madin-Darby canine kidney (MDCK) cells, with a Ki value of 11 nM. [1]
NET inhibition: Reboxetine mesylate (0.1–100 nM) dose-dependently inhibited [³H]-norepinephrine uptake in HEK293 cells overexpressing human NET, achieving 95% inhibition at 50 nM; no significant inhibition of [³H]-serotonin uptake (SERT) or [³H]-dopamine uptake (DAT) at concentrations up to 1 μM [5] - Neuronal activity modulation: In rat cortical slices, 1–10 μM increased extracellular norepinephrine levels by 2.3–4.8-fold (microdialysis + HPLC), without affecting serotonin or dopamine levels [4] - No cytotoxicity: CC₅₀ > 100 μM in PC12 cells and primary rat cortical neurons; cell viability >90% at concentrations up to 50 μM (MTT assay) [5] |
| ln Vivo |
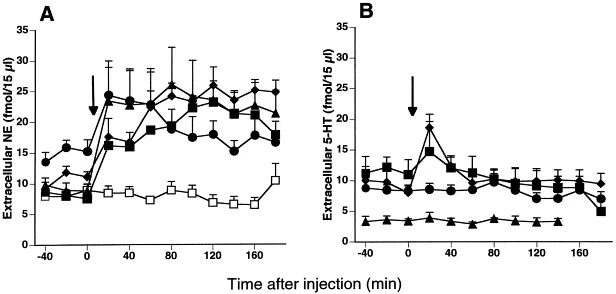
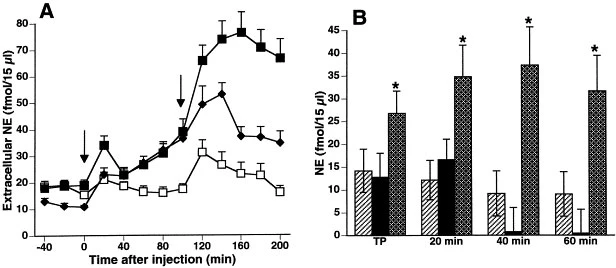
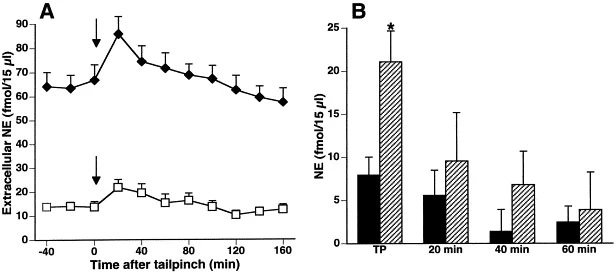
Reboxetine potently and dose-dependently inhibits the firing of locus coeruleus neurons in rats with ED50 of 191 μg/kg. Piperoxan (1.5 mg/kg, IV), an α2 antagonist, can reverse the effects of reboxetine-induced inhibition of locus coeruleus neurons. The mice's blepharospasm and hypothermia caused by reserpine are reversed by reboxetine in a dose-dependent manner. Additionally, it is discovered that reboxetine counteracts the dose-dependent hypothermia in mice induced by clonidine. In rats, reboxetine (ED50 = 10 mg/kg and 3 mg/kg (p.o.)) reverses blepharospasm and hypothermia caused by reserpine.[1] In patients with DSM-III-R panic disorder, reboxetine significantly lowers the mean number of panic attacks and phobic symptoms. Additionally, reboxetine improves scores on the Sheehan Disability Scale, Hopkins Symptom Checklist-90, and Hamilton Rating Scale for Depression.[2] In patients with recurrent DSM-III-R major depression, reboxetine is linked to a significantly lower relapse rate than placebo (22% vs. 56%) and a higher cumulative probability of a maintained response during long-term treatment. After an episode ends, reboxetine effectively prevents depression symptoms from returning.[3] Reboxetine (0.3 mg/kg–20 mg/kg) administered systemically to rats dose-dependently raises extracellular norepinephrine in the frontal cortex, but has no effect on extracellular serotonin. The rat frontal cortex's extracellular dopamine is also increased by reboxetine (20 mg/kg). When Reboxetine is administered chronically for 14 days, the rat frontal cortex exhibits increased basal concentrations of extracellular norepinephrine and dopamine as well as a greater net increase in these substances—but not serotonin.[4] Reboxetine dose-dependently reduces the self-administration of nicotine by approximately 60%. Reboxetine (5.6 mg/kg) is administered repeatedly over the course of 14 sessions, which reduces nicotine self-administration and sucrose-maintained responding.[5]
Antidepressant-like activity (mouse models): Oral administration of Reboxetine mesylate (5, 10, 20 mg/kg) dose-dependently reduced immobility time in the forced swim test (FST) by 32%, 55%, and 68% respectively, and in the tail suspension test (TST) by 28%, 48%, and 62% compared to vehicle [1][4] - Norepinephrine level elevation: In rat brain (prefrontal cortex, hippocampus), oral 10 mg/kg increased tissue norepinephrine content by 1.8-fold and 2.1-fold respectively (HPLC) [4] - Clinical antidepressant efficacy: In patients with major depressive disorder (MDD), oral Reboxetine mesylate (4–8 mg/day, twice daily) for 6–8 weeks improved Montgomery-Åsberg Depression Rating Scale (MADRS) scores by 35–52% (responders rate: 58–65%) [2][3] - No significant effect on cardiovascular parameters: In conscious rats, intravenous 5 mg/kg did not alter heart rate or blood pressure [5] |
| Enzyme Assay |
NET radioligand binding assay: Recombinant human NET protein was immobilized on membranes. Serial dilutions of Reboxetine mesylate (0.01 nM–1 μM) were incubated with [³H]-nisoxetine (NET-specific ligand) at 25°C for 60 minutes. Bound and free ligands were separated by filtration, and radioactivity was quantified to calculate Ki value [5]
- Norepinephrine uptake inhibition assay: HEK293 cells overexpressing human NET were seeded in 24-well plates, pretreated with Reboxetine mesylate (0.1 nM–1 μM) for 30 minutes, then incubated with [³H]-norepinephrine for 15 minutes at 37°C. Cells were washed, lysed, and radioactivity was measured to assess uptake inhibition and IC₅₀ [5] |
| Cell Assay |
Cell Line: SH-SY5Y cells
Concentration: 0.1 μM, 1 μM, 5 μM Incubation Time: 24 hours Result: Prevented the Dexamethasone-induced decreases in cell viability and proliferation rate. NET-mediated uptake assay in transfected cells: HEK293 cells were transfected with human NET cDNA, cultured for 48 hours, and serum-starved for 1 hour. Cells were treated with Reboxetine mesylate (0.1–100 nM) and [³H]-norepinephrine, followed by lysis and radioactivity quantification [5] - Primary cortical neuron assay: Rat cortical neurons were cultured for 7–10 days, treated with Reboxetine mesylate (1–10 μM) for 24 hours. Extracellular fluid was collected, and norepinephrine levels were measured by HPLC to confirm neurotransmitter release/uptake modulation [4] |
| Animal Protocol |
Harlan-bred, male CF-1 mice (18-20 g), depression models
3 mg/kg, 30 mg/kg Intraperitoneal injection Mouse FST/TST models: Male CD-1 mice (20–25 g) were orally administered Reboxetine mesylate (5, 10, 20 mg/kg) 60 minutes before the forced swim test (6-minute session) or tail suspension test (6-minute session). Immobility time was recorded and analyzed [1][4] - Rat microdialysis model: Male Sprague-Dawley rats (250–300 g) were implanted with microdialysis probes in the prefrontal cortex. After recovery, Reboxetine mesylate (10 mg/kg, oral) was administered, and dialysates were collected every 20 minutes for 4 hours. Norepinephrine levels were quantified by HPLC [4] - Drug formulation: Reboxetine mesylate was dissolved in distilled water for oral administration; for intravenous injection, it was dissolved in physiological saline [4][5] |
| ADME/Pharmacokinetics |
Oral bioavailability: 76% (rat, 10 mg/kg orally); 85% (human, 4 mg orally) [5]
- Half-life (t₁/₂): 6.2 hours (rat, intravenous); 12.5 hours (human, orally) [5] - Volume of distribution (Vd): 2.8 L/kg (rat, intravenous); 3.1 L/kg (human, intravenous) [5] - Metabolism: Primarily metabolized in the liver by cytochrome P450 3A4 (CYP3A4) to inactive metabolites [2][5] - Excretion: 65% in urine (current drug + metabolites); 25% in feces [5] |
| Toxicity/Toxicokinetics |
Effects During Pregnancy and Lactation
◉ Overview of Use During Lactation Reboxetine has not been approved for marketing by the U.S. Food and Drug Administration (FDA), but it is available in other countries. Limited information suggests that even with daily doses up to 10 mg, low concentrations of the drug in breast milk do not appear to have any adverse effects on breastfed infants. Breastfeeding women should be closely monitored for reboxetine use until more data become available. ◉ Effects on Breastfed Infants Four infants whose mothers had postpartum depression were breastfed for 1.3 to 2.1 months (feeding duration not specified) while their mothers were receiving reboxetine treatment (mean daily dose of 6.5 mg (79 mcg/kg)). One mother was also taking 20 mg of escitalopram daily, and another was taking 300 mg of sertraline daily. No adverse reactions were observed in any of the infants. Three of the infants had normal Denver developmental scores; the fourth infant, whose mother was taking reboxetine, had a developmental age of only 71% of normal, but this problem existed before the mother started taking reboxetine. Five women took reboxetine during pregnancy and lactation (time of use not specified), at unknown dosages. Their infants experienced no adverse reactions and all developmental milestones were normal. ◉ Effects on Lactation and Breast Milk Reboxetine increases serum prolactin levels in male subjects. The significance of this finding for lactating mothers is unclear. For mothers who have established lactation, prolactin levels may not affect their ability to breastfeed. An observational study investigated the outcomes of 2,859 women who took antidepressants for two years prior to pregnancy. Compared to women who did not take antidepressants during pregnancy, mothers who took antidepressants during all three stages of pregnancy were 37% less likely to breastfeed at discharge. Mothers who took antidepressants only in the third trimester were 75% less likely to breastfeed at discharge. Mothers who took antidepressants only in the first and second trimesters were not less likely to breastfeed at discharge. The study did not specify the type of antidepressant used by the mothers. A retrospective cohort study analyzed hospital electronic medical records from 2001 to 2008, comparing women who took antidepressants in late pregnancy (n = 575), women with mental illness but not taking antidepressants (n = 1552), and mothers not diagnosed with mental illness (n = 30,535). Women treated with antidepressants were 37% less likely to breastfeed at discharge than women not diagnosed with mental illness, but there was no difference in the likelihood of breastfeeding compared to untreated mothers diagnosed with mental illness. None of the mothers were taking reboxetine. A study of 80,882 Norwegian mother-infant pairs between 1999 and 2008 showed that 392 women reported starting antidepressants postpartum, and 201 women reported starting antidepressants during pregnancy. Compared to the control group who were not exposed to antidepressants, taking antidepressants in late pregnancy was associated with a 7% lower likelihood of initiating breastfeeding, but had no effect on the duration of breastfeeding or the rate of exclusive breastfeeding. Compared to the control group who were not exposed to antidepressants, starting or restarting antidepressants was associated with a 63% lower likelihood of primary breastfeeding at 6 months, a 51% lower likelihood of any breastfeeding, and a 2.6-fold increased risk of abruptly stopping breastfeeding. No specific antidepressant was mentioned. Plasma protein binding rate: 97% (human plasma, ultrafiltration) [5] -In vitro toxicity: CC₅₀ in PC12 cells and primary cortical neurons > 100 μM [5] -Clinical side effects: In patients with MDD (4-8 mg/day, 6-8 weeks), common adverse reactions included dry mouth (28%), constipation (22%), insomnia (18%) and sweating (15%) [2][3] -Acute toxicity in animals: LD₅₀ > 200 mg/kg (mice, oral); no death or obvious toxic symptoms were observed at doses up to 150 mg/kg [5] |
| References | |
| Additional Infomation |
morpholine derivative is a selective and potent norepinephrine reuptake inhibitor; used to treat depression.
Reboxetine mesylate is a selective, potent, and reversible norepinephrine reuptake inhibitor (NRI) [1][5] - Its mechanism of action includes blocking NET-mediated norepinephrine reuptake to presynaptic neurons, thereby increasing norepinephrine levels in the synaptic cleft and exerting an antidepressant effect [1][4] - It has been clinically approved for the treatment of major depressive disorder (MDD); it can effectively improve mood, anhedonia, and psychomotor retardation in patients with major depressive disorder [2][3] - It has no significant affinity for muscarinic receptors, histamine receptors, or serotonin receptors, and compared with tricyclic antidepressants, it can minimize anticholinergic and sedative side effects [5] |
| Molecular Formula |
C20H27NO6S
|
|---|---|
| Molecular Weight |
409.5
|
| Exact Mass |
409.155
|
| Elemental Analysis |
C, 58.66; H, 6.65; N, 3.42; O, 23.44; S, 7.83
|
| CAS # |
98769-84-7
|
| Related CAS # |
Reboxetine; 71620-89-8; (R,R)-Reboxetine mesylate; 105017-39-8
|
| PubChem CID |
127150
|
| Appearance |
White to off-white solid powder
|
| Boiling Point |
443.7ºC at 760 mmHg
|
| Melting Point |
170-171ºC
|
| Flash Point |
188.2ºC
|
| LogP |
4.107
|
| Hydrogen Bond Donor Count |
2
|
| Hydrogen Bond Acceptor Count |
7
|
| Rotatable Bond Count |
6
|
| Heavy Atom Count |
28
|
| Complexity |
425
|
| Defined Atom Stereocenter Count |
2
|
| SMILES |
S(C([H])([H])[H])(=O)(=O)O[H].O1C([H])([H])C([H])([H])N([H])C([H])([H])[C@]1([H])[C@@]([H])(C1C([H])=C([H])C([H])=C([H])C=1[H])OC1=C([H])C([H])=C([H])C([H])=C1OC([H])([H])C([H])([H])[H]
|
| InChi Key |
CGTZMJIMMUNLQD-STYNFMPRSA-N
|
| InChi Code |
InChI=1S/C19H23NO3.CH4O3S/c1-2-21-16-10-6-7-11-17(16)23-19(15-8-4-3-5-9-15)18-14-20-12-13-22-18;1-5(2,3)4/h3-11,18-20H,2,12-14H2,1H3;1H3,(H,2,3,4)/t18-,19-;/m1./s1
|
| Chemical Name |
(2R)-2-[(R)-(2-ethoxyphenoxy)-phenylmethyl]morpholine;methanesulfonic acid
|
| Synonyms |
PNU 155950E; PNU155950E; PNU-155950E; FCE-20124 mesylate; PNU-155950E mesylate; FCE 20124 mesylate; PNU 155950E mesylate; FCE20124 mesylate; PNU155950E mesylate; Reboxetine mesilate; Reboxetine; Edronax; Reboxetine mesylate; Vestra (TN); AC1L2RIX; AC1Q6WCV; DSSTox_CID_25690; DSSTox_RID_81062; DSSTox_GSID_45690.
|
| HS Tariff Code |
2934.99.9001
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: Please store this product in a sealed and protected environment, avoid exposure to moisture. |
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
DMSO: 82~125 mg/mL (200.2~305.3 mM)
Water: < 1 mg/mL Ethanol: ~82 mg/mL (~200.2 mM) |
|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.08 mg/mL (5.08 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution.
For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 20.8 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.08 mg/mL (5.08 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 20.8 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. View More
Solubility in Formulation 3: ≥ 2.08 mg/mL (5.08 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. Solubility in Formulation 4: 110 mg/mL (268.62 mM) in PBS (add these co-solvents sequentially from left to right, and one by one), clear solution; with ultrasonication. |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 2.4420 mL | 12.2100 mL | 24.4200 mL | |
| 5 mM | 0.4884 mL | 2.4420 mL | 4.8840 mL | |
| 10 mM | 0.2442 mL | 1.2210 mL | 2.4420 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
|
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved





























 COA
COA