| Size | Price | Stock | Qty |
|---|---|---|---|
| 500mg |
|
||
| 1g |
|
||
| 2g |
|
||
| 5g |
|
||
| Other Sizes |
































Purity: ≥98%
Isotretinoin (Accutane; Myorisan; Zenatane; 13-cis retinoic acid) is a topically used medication approved for the treatment of severe cystic acne. It was originally developed to be used as a chemotherapeutic drug for the treatment of various cancers such as brain cancer, pancreatic cancer etc. Isotretinoin directly interferes with the development of cranial neural crest cells. Isotretinoin selectively affects neural crest cells by decreasing their cell-substratum adhesion. Isotretinoin (500 ng/mL) and its main metabolite in the human, 4-oxo-isotretinoin, induce malformations similar to those seen in vivo.
| Targets |
Isotretinoin exerts effects by binding to retinoic acid receptors (RARα, RARβ, RARγ) [1]
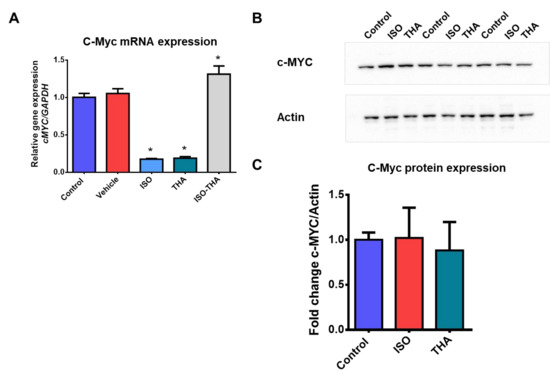
- Isotretinoin down-regulates the expression of the c-MYC gene, which is considered a relevant target for its anti-cancer-related activity [4] |
|---|---|
| ln Vitro |
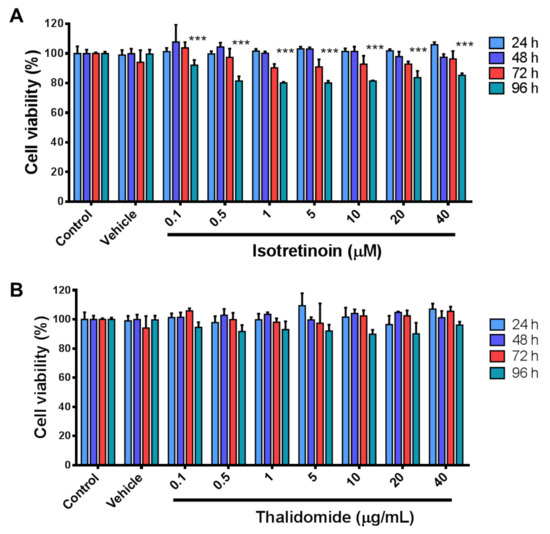
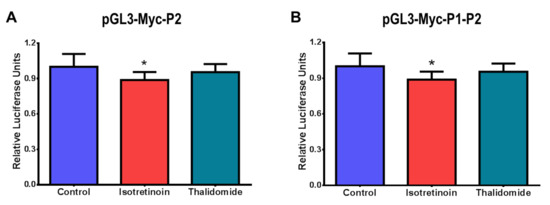
As a prodrug, isotretinoin (13-cis-retinoic acid) is transformed intracellularly into metabolites that agonistically bind to the nuclear receptors RAR and RXR [1]. The sensitivity of isotretinoin to light, heat, and air is quite great [3]. HepG2 cell viability is considerably inhibited by isotretinoin (0–40 μM; 24-96 hours) [4]. P1 or P2 promoter activity contributes to the downregulation of c-MYC mRNA expression caused by isotretinoin (10 μM; 48 hours) [4].
In human hepatic cells (HepG2), treatment with isotretinoin (concentration not specified) resulted in a significant down-regulation of c-MYC gene expression, as detected by quantitative polymerase chain reaction (qPCR). Western blot analysis further showed that isotretinoin modified the expression levels of proteins associated with cancer progression in these cells, including a decrease in proteins promoting cell proliferation and an increase in proteins involved in cell cycle regulation (specific protein names and fold changes not detailed) [4] |
| ln Vivo |
When administered inhalation for 45 minutes daily for two weeks, isotretinoin (1.3–481 μg/L; also known as 13-cis-retinoiic acid) can effectively prevent lung cancer in A/J mice [2]. In rats, isotretinoin speeds up alveolar healing following tooth extraction [3].
In A/J mice (a strain susceptible to lung tumorigenesis), inhaled isotretinoin at low doses (specific dose: 0.1 mg/kg body weight, administered via inhalation) exhibited effective chemopreventive activity against lung cancer. Compared to the control group (mice not treated with isotretinoin), the treated group showed a significant reduction in the number of lung tumors (average tumor number reduced by approximately 40%, exact values not fully specified) and a decrease in tumor size after a treatment period of 16 weeks [2] - In rats undergoing exodontia (tooth extraction), oral administration of isotretinoin (dose: 2 mg/kg body weight, given daily) promoted alveolar repair. Histological analysis of alveolar bone tissue at 7 and 14 days post-tooth extraction revealed that the isotretinoin-treated group had increased osteoblastic activity, enhanced collagen deposition, and accelerated formation of new bone tissue compared to the control group (rats receiving vehicle only) [3] |
| Cell Assay |
Cell Viability Assay[4]
Cell Types: HepG2 Tested Concentrations: 0.1, 0.5, 1, 5, 10, 20, and 40 μM Incubation Duration: 24, 48, 72, and 96 h Experimental Results: demonstrated a significant reduction in cell viability (less than 30%) at 96 h for all doses. RT-PCR[4] Cell Types: HepG2 Tested Concentrations: 10 µM Incubation Duration: 48 h Experimental Results: Dramatically decreased the expression of c-MYC mRNA by ~80%. HepG2 cells (human hepatic cells) were cultured in a suitable medium (composition not detailed) under standard conditions (37°C, 5% CO₂). Cells were seeded in culture plates and allowed to attach for 24 hours before treatment. Isotretinoin was dissolved in an appropriate solvent (solvent type not specified) and added to the cell culture medium at a final concentration for a treatment duration of 48 hours. After treatment, cells were harvested; total RNA was extracted for qPCR analysis to detect c-MYC gene expression, and total protein was extracted for Western blot analysis to determine the levels of cancer-associated proteins (specific proteins include those involved in cell proliferation and cycle regulation, with detection procedures following standard qPCR and Western blot protocols: reverse transcription of RNA to cDNA, PCR amplification with specific primers for c-MYC, protein separation by SDS-PAGE, transfer to membranes, incubation with primary and secondary antibodies, and detection by chemiluminescence) [4] |
| Animal Protocol |
Animal/Disease Models: Male A/J mice, lung carcinogenesis model[2]
Doses: 1.3, 20.7, or 481 μg/L Route of Administration: Inhalation exposure, 45 min daily for 2 weeks Experimental Results: decreased the tumor multiplicity. Caused up-regulation of lung tissue nuclear retinoic acid receptors (RARs) relative to vehicle-exposed mice, RARα (3.9-fold vehicle), RARβ (3.3-fold), and RARγ (3.7-fold) at 20.7 μg/L. Animal/Disease Models: Wistar rats, tooth extraction model[3] Doses: 7.5 mg/kg Route of Administration: po (oral gavage), daily for 30 days Experimental Results: Accelerated the process of alveolar repair, Dramatically diminished serum calcium levels. For the lung cancer chemopreventive study in A/J mice: Mice (female, 6-8 weeks old) were housed under specific pathogen-free (SPF) conditions with a 12-hour light/dark cycle, free access to food and water. Isotretinoin was formulated as an inhalable aerosol. Mice were exposed to inhaled isotretinoin at a dose of 0.1 mg/kg body weight, with inhalation sessions conducted once daily, 5 days a week, for a total treatment period of 16 weeks. Before the start of isotretinoin treatment, mice were administered a lung tumor initiator to induce tumor formation. At the end of the treatment period, mice were euthanized, and their lungs were removed, fixed in formalin, and sectioned for histological examination to count the number of lung tumors [2] - For the alveolar repair study in rats: Male Wistar rats (200-250 g body weight) were housed in a controlled environment (temperature 22±2°C, 12-hour light/dark cycle) with free access to food and water. Isotretinoin was dissolved in corn oil (solvent) to prepare a solution with a concentration of 0.2 mg/mL. Rats were divided into two groups: the treatment group received oral gavage of isotretinoin at a dose of 2 mg/kg body weight once daily, and the control group received oral gavage of an equal volume of corn oil. Treatment started 3 days before tooth extraction and continued for 14 days after extraction. On the day of tooth extraction, rats were anesthetized (anesthetic type not specified), and the right maxillary first molar was extracted. At 7 and 14 days post-extraction, rats were euthanized, and the maxillary bone containing the extraction socket was harvested, fixed in 10% formalin, decalcified, embedded in paraffin, sectioned, and stained with hematoxylin-eosin (HE) for histological evaluation of alveolar repair [3] |
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion
Following oral administration of 100 mg isotretinoin, peak plasma concentrations (74-511 ng/mL) are reached within 1-4 hours. Isotretinoin is better absorbed when taken with a high-fat meal, and bioavailability may vary between different brands. In fasting subjects, after oral administration of 40 mg isotretinoin, peak plasma concentrations (314 ng/mL) were reached within 2.9 hours, with an area under the curve (AUC) of 4055 ng/mL·h. In subjects who took 40 mg isotretinoin after a high-fat meal, peak plasma concentrations (395 ng/mL) were reached within 6.4 hours, with an AUC of 6095 ng/mL·h. Isotretinoin and its metabolites are excreted in urine and feces as conjugates, with similar excretion rates. 53-74% of oral isotretinoin is excreted unchanged in feces. Since there is currently no intravenous formulation, the volume of distribution in the human body is unknown. A study of children with neuroblastoma found that the volume of distribution (VOD) of isotretinoin was 85 liters. In guinea pigs, the VOD was 2432 ml/kg, and in obese rats, it was 1716 ml/kg. The clearance rate of isotretinoin in children with neuroblastoma was 15.9 L/h. In guinea pigs, the clearance rate was 21.3 ml/min/kg, and in obese rats, it was 7.2 ml/min/kg. After oral administration of isotretinoin, there is a significant delay of approximately 0.5–2 hours before the drug enters systemic circulation. This delay is believed to be due to capsule disintegration and subsequent dissolution of the drug in the gastrointestinal contents. After this delay, absorption is rapid. The actual bioavailability of oral isotretinoin in humans has not been determined, but animal studies suggest that approximately 25% of the oral dose enters systemic circulation unchanged. The low bioavailability observed in animals is likely due to biodegradation of the drug in the gastrointestinal tract and/or during absorption (in the gastrointestinal mucosa) and first-pass metabolism in the liver. Food and/or milk increase the gastrointestinal absorption of isotretinoin. Compared with fasting, peak plasma concentrations are slightly delayed but significantly increased when isotretinoin is taken 1 hour before, during, or after a meal, with an area under the plasma concentration-time curve (AUC) of approximately 1.5–2 times. Due to its high lipophilicity, isotretinoin's oral absorption can be enhanced when taken with high-fat foods. In a crossover study, 74 healthy adults took a single dose of 80 mg isotretinoin (two 40 mg capsules) in both fasting and postprandial states. The results showed that, compared with fasting, taking a standard high-fat meal immediately after a meal more than doubled both the peak plasma concentration and the area under the plasma concentration-time curve (AUC) of isotretinoin. Since the observed elimination half-life remained unchanged, it is suggested that food may enhance the bioavailability of isotretinoin without altering its distribution in the body. Food also prolongs the time to peak concentration, which may be related to the prolonged absorption period. Therefore, the manufacturer recommends that isotretinoin capsules should always be taken with food. The combined mean elimination time of isotretinoin administered intravenously and orally was approximately 5.5 hours. The mean plasma clearance after intravenous administration and the intrinsic clearance after oral administration were 5.19 and 6.63 mL/min/kg, respectively. The mean absorbed bioavailability was approximately 21%, indicating a first-pass effect of approximately 80%. Analysis of total (14)-C activity in intestinal contents indicated that a portion of the isotretinoin dose undergoes bio or chemical degradation in the intestinal lumen before absorption. The clinical dose range of isotretinoin is 0.5 to 8 mg/kg/day, with acute side effects occurring at doses of 1 mg/kg/day or higher. Following single or multiple doses, isotretinoin plasma concentrations peak within 2 to 4 hours, with an elimination half-life of 10 to 20 hours. The plasma concentration-time curves of isotretinoin after single or multiple dosing regimens can be well described by a linear model exhibiting a biphasic distribution. In most cases, retinoids achieve maximum efficacy within approximately 8 weeks (at the highest tolerated dose), and symptoms typically recur slowly over several weeks after discontinuation—except in cases of isotretinoin treatment for cystic acne. Maintenance or intermittent dosing can generally prolong remission. This article discusses a case study involving the distribution of 13-cis-retinoic acid in embryonic tissue following an accidental administration of 40 mg/day of isotretinoin by a woman during days 8 to 28 of pregnancy. Pregnancy terminated on day 31, and maternal serum samples were collected between 72 and 80 hours after the last dose of isotretinoin. The concentrations of retinoic acid in maternal serum, embryonic tissue, and six placental tissue samples were then determined using high-performance liquid chromatography (HPLC). The results showed that, contrary to previous findings in mice, isotretinoin intake during pregnancy in humans leads to increased all-trans retinoic acid concentrations in the placenta and embryo. This leads to the conclusion that metabolic activation of isotretinoin to its all-trans isomer may be the cause of its teratogenicity. For more complete data on the absorption, distribution, and excretion of 13-cis retinoic acid (11 in total), please visit the HSDB record page. Metabolites/Metabolites Isotretinoin, or 13-cis retinoic acid, can undergo reversible cis-trans isomerization to produce all-trans retinoic acid. Isotretinoin is 4-hydroxylated to 4-hydroxy-13-cis retinoic acid, which is then oxidized to the major metabolite 4-oxo-13-cis retinoic acid. All-trans retinoic acid is 4-hydroxylated to 4-hydroxy-all-trans retinoic acid, which is then oxidized to 4-oxo-all-trans retinoic acid. 4-oxo-13-cis-retinoic acid can undergo reversible cis-trans isomerization to produce 4-oxo-all-trans-retinoic acid. In human volunteers and patients, one of the main blood metabolites of isotretinoin is 4-oxo-isotretinoin, which is cleared more slowly than isotretinoin and may itself be involved in teratogenic processes. This review summarizes the teratogenicity of isotretinoin, focusing on species differences, toxicokinetics, and metabolism. Species insensitive to isotretinoin (rats, mice) rapidly clear the drug through detoxification to β-glucuronide; furthermore, placental transport in these species is limited. On the other hand, in species sensitive to isotretinoin (primates), the drug is primarily metabolized to the active ingredient 13-cis-4-oxo-retinoic acid; placental transport is more extensive in these species. In all tested species, placental transport of β-glucuronide was limited; these metabolites were present at extremely low concentrations in humans, sometimes undetectable. 13-cis-retinoic acid (13-retinoic acid) did not bind significantly to cellular retinoid-binding proteins or nuclear receptors, and its tissue distribution and placental transport were also low. Its entry into the cell nucleus is likely significant. Due to the long half-life of 13-cis-retinoic acid, persistent isomerization led to a significant increase in the area under the concentration-time curve (AUC) of all-trans-retinoic acid in mice, monkeys, and humans; the resulting all-trans-retinoic acid was widely distributed in the placenta and may be an important factor in the teratogenic effects of 13-cis-retinoic acid. Isomerization could not explain the teratogenic effects of 13-cis-retinoic acid in rats and rabbits. The conclusion is that isotretinoin exhibits high teratogenic activity in susceptible species (humans and monkeys), which is related to the slow elimination of the 13-cis isomer, metabolism to a 4-oxo derivative, increased placental transport, persistent isomerization, and significant exposure of target tissues to all-trans retinoic acid. Furthermore, isotretinoin lacks binding to cytoplasmic retinoid-binding proteins, which may facilitate its entry into the cell nucleus. Isotretinoin is primarily metabolized in the liver via the cytochrome P-450 (CYP) microsomal enzyme system, mainly catalyzed by CYP2C8, CYP2C9, CYP3A4, and CYP2B6 isoenzymes, generating various metabolites (e.g., 4-oxoisotretinoin, retinoic acid [retinoic acid], and 4-oxoretinoic acid [4-oxoretinoic acid]). Retinoic acid and 13-cis retinoic acid are geometric isomers that can reversibly convert to each other; administration of one isomer will generate the other isomer. Isotretinoin is also irreversibly oxidized to 4-oxoisotretinoin, which generates its geometric isomer, 4-oxoretinoic acid ketone. All these metabolites exhibit higher retinoid activity than the parent compound in certain in vitro models. However, the clinical significance of these models remains unclear. Studies have shown that taking isotretinoin with food increases the production of all metabolites in plasma compared to fasting. Furthermore, patients' steady-state exposure to 4-oxoisotretinoin is approximately 3.4 times that of isotretinoin under both fasting and eating conditions. In vitro studies have shown that the major P450 isoenzymes involved in isotretinoin metabolism are 2C8, 2C9, 3A4, and 2B6. Isotretinoin and its metabolites are further metabolized into conjugates and then excreted in urine and feces. For more complete metabolite/metabolite data on 13-cis-retinoic acid (6 metabolites), please visit the HSDB record page. The known human metabolites of isotretinoin include (2Z,4E,6Z,8E)-6-hydroxy-3,7-dimethyl-9-(2,6,6-trimethylcyclohexen-1-yl)non-2,4,6,8-tetraenoic acid. Biological half-life The half-life ranges from 7 to 39 hours, with a mean elimination half-life of 20 hours. The half-life of 4-oxo-13-cis-retinoic acid is 17 to 50 hours, with a mean elimination half-life of 25 hours. After oral administration of 80 mg of (14)C-isotretinoin liquid suspension, the activity of (14)C in the blood decreased, with a half-life of 90 hours. In 74 healthy adult subjects, after a single oral dose of 80 mg isotretinoin while in a food-treated state, the mean elimination half-lives ± standard deviations for isotretinoin and 4-oxo-isotretinoin were 21 ± 8.2 hours and 24 ± 5.3 hours, respectively. Isotretinoin plasma concentrations exhibited a biphasic decline. In adults with normal renal function, the mean initial phase half-life was 0.5 hours, and the mean terminal phase half-life was 10–20 hours (range: 7–39 hours). …After single and multiple administrations, peak plasma concentrations of isotretinoin were reached between 2 and 4 hours, with elimination half-lives of 10–20 hours… For more complete biological half-life data for 13-cis-retinoic acids (6 in total), please visit the HSDB records page. |
| Toxicity/Toxicokinetics |
Hepatotoxicity
Up to 15% of patients taking isotretinoin experience abnormal liver function, but significant increases in liver function indicators exceeding three times the upper limit of normal or requiring discontinuation of the drug are rare (Probability Score: D (likely to cause clinically significant liver damage in rare cases)). Use during Pregnancy and Lactation ◉ Overview of Use During Lactation There is currently no information regarding the use of isotretinoin during lactation. During lactation, especially with newborns or premature infants, it may be more common to use topical medications that are not easily absorbed by the mother. ◉ Effects on Breastfed Infants As of the revision date, no relevant published information was found. ◉ Effects on Lactation and Breast Milk A woman who had weaned 18 months prior experienced nipple discharge from her right breast after 5.5 months of isotretinoin treatment. Nipple discharge occurred after taking isotretinoin. Microbiological, hormonal (including prolactin), radiological and physical examination results were all normal. Nipple discharge stopped one month after isotretinoin was discontinued. Nipple discharge recurred within 10 days after the same dose of isotretinoin was resumed. [1] Galactorrhea may be caused by isotretinoin. A review of adverse reaction reports of gynecomastia caused by retinoids submitted by the French Pharmacovigilance Center found that 22 cases of gynecomastia were associated with the use of isotretinoin. Of these, 14 were gynecomastia, 6 were galactorrhea, and 2 had both gynecomastia and galactorrhea. In the reported cases of retinoids, nearly half of the gynecomastia and/or galactorrhea were unilateral. The median time to onset was 90 days (interquartile range 39 to 347 days). Of the 31 patients, 27 had known treatment outcomes, and 63% of the patients recovered completely after discontinuation of retinoic acid. [2] ◈ What is isotretinoin? Isotretinoin is a prescription, oral medication used to treat severe cystic acne that has not responded to other treatments. Isotretinoin is a derivative of vitamin A. It has been marketed under various brand names, such as Accutane®, Absorica®, Amnesteem®, Claravis®, Eprilis®, Clarus®, Myorisan®, Sotret®, and Zenatane®. Isotretinoin product labels advise against its use during pregnancy. This is because isotretinoin use during pregnancy may lead to birth defects and other pregnancy-related problems. If you are taking isotretinoin and find out you are pregnant, stop taking it immediately and contact your healthcare provider. If you are taking isotretinoin and are planning to become pregnant, discuss your medication use, your condition, and the best treatment option for you with your healthcare provider. ◈ I am taking isotretinoin. Will it affect my ability to conceive? People trying to conceive should not take isotretinoin. There are reports of some people experiencing changes in their menstrual cycle (menstrual period) while taking isotretinoin. There are currently no reports of isotretinoin affecting pregnancy. ◈ I'm taking isotretinoin, but I want to stop before getting pregnant. How long will it stay in my body? Everyone metabolizes the drug at a different rate. For healthy adults, it takes an average of about 6 days to clear most of the isotretinoin from the body. However, it is recommended to wait one month after stopping isotretinoin before trying to conceive. ◈ I just found out I'm pregnant. Should I stop taking isotretinoin? Yes, if you find out you are pregnant, it is recommended that you stop taking isotretinoin immediately. If you are pregnant, contact the healthcare provider who prescribed your isotretinoin and the healthcare provider responsible for your care during your pregnancy as soon as possible. Isotretinoin may cause birth defects. Your medical team can discuss the risks of this medication to your pregnancy and possible treatment options with you. ◈ Does taking isotretinoin increase the risk of miscarriage? Miscarriage is common and can occur in any pregnancy for a variety of reasons. Taking isotretinoin increases the risk of miscarriage. If isotretinoin is taken in early pregnancy, the risk of miscarriage can be as high as 40%. ◈ Does taking isotretinoin increase the risk of birth defects? There is a 3-5% risk of birth defects in each pregnancy, known as the baseline risk. Isotretinoin can cause birth defects in up to 35% or more of babies who are exposed to the drug during pregnancy. Even with short-term use, it is still possible to have a baby with birth defects. In the short term, most babies with birth defects will have microtia or missing auricles, as well as hearing and vision problems. Other reported problems include: heart defects, hydrocephalus, micrognathia, microcephaly, cleft palate (the opening at the top of the mouth), and malformation or absence of the thymus (a hormone-secreting gland). While not all pregnant women exposed to isotretinoin will develop birth defects, it is recommended that pregnant women avoid using isotretinoin. ◈ Does taking isotretinoin during pregnancy increase the risk of other pregnancy-related problems? Using isotretinoin during pregnancy increases the risk of premature birth (delivery before 37 weeks of gestation). ◈ Will taking isotretinoin during pregnancy affect a child's future behavior or learning? Children exposed to isotretinoin during pregnancy may experience hearing and vision problems, which can lead to learning disabilities. Children exposed to isotretinoin may also experience moderate to severe behavioral problems and/or intellectual disabilities. These problems are often not detected at birth but develop gradually as the child grows. Other potential long-term effects of isotretinoin exposure during pregnancy on children are not yet clear. ◈ What screenings or tests can determine if I have birth defects or other problems during my pregnancy? Prenatal ultrasound can be used to screen for certain birth defects. Ultrasound can also be used to monitor fetal growth and development. Please consult your healthcare provider about any prenatal screenings or tests you can have. Currently, there are no tests during pregnancy that can predict the extent of isotretinoin's impact on future behavior or learning abilities. ◈ Can I still get a prescription for isotretinoin? Isotretinoin can be prescribed through a special program called the iPLEDGE® Risk Assessment and Mitigation Strategy (REMS). People must comply with all the requirements of this program to obtain a prescription for isotretinoin. Here are some requirements: You must discuss isotretinoin and the iPLEDGE® REMS plan with your healthcare provider. You must understand that isotretinoin use may cause serious birth defects. You must receive and understand the safety information about isotretinoin and the requirements of the iPLEDGE® REMS plan. You must be enrolled in the iPLEDGE® REMS plan by your healthcare provider within 30 days before your first prescription. You must read, understand, and sign the informed consent form containing warnings about the risks of isotretinoin use. You must correctly answer the comprehensive questions on the iPLEDGE® REMS plan website. You must not be pregnant, planning to become pregnant, or breastfeeding. Two negative pregnancy tests are required before starting isotretinoin. A pregnancy test must be performed monthly during treatment. A negative pregnancy test is required before each prescription. You must always use two different methods of contraception (unless you agree to abstain from sexual intercourse), starting one month before treatment, continuing during treatment, and continuing for one month after treatment. You must pick up your medication within 7 days of your appointment. You must agree to monthly appointments for health checks and to obtain new prescriptions during treatment. Do not share medication with others. Do not donate blood during treatment and for one month after treatment ends. For more information about the iPLEDGE program, please call 1-866-495-0654 or visit the iPLEDGE website at https://www.ipledgeprogram.com. Even if you are not sexually active or planning to become pregnant, it is recommended that you consult a healthcare provider if you are using or want to use isotretinoin. Using effective contraception is very important, as nearly 50% of pregnancies are unplanned or unintended. ◈ Breastfeeding while taking isotretinoin: Isotretinoin product labels advise against using this medication while breastfeeding. There are currently no studies on the use of isotretinoin while breastfeeding. It is unknown what effects (if any) isotretinoin exposure through breast milk may have on a breastfeeding infant. Please consult your healthcare provider if you have any questions about breastfeeding. ◈ Does the use of isotretinoin by men affect fertility or increase the risk of birth defects? A few reports have indicated that men taking isotretinoin may experience erectile dysfunction (difficulty achieving or maintaining an erection) and ejaculatory dysfunction (inability to ejaculate). This may affect fertility (the ability to impregnate a partner). No studies have yet explored whether isotretinoin increases the risk of birth defects in male fetuses. Generally, contact with the father or sperm donor is unlikely to increase the risk of pregnancy. For more information, please see the "Fatherly Exposure to Isotretinoin" information sheet on the MotherToBaby website: https://mothertobaby.org/fact-sheets/paternal-exposures-pregnancy/. Protein BindingIsotretinoin has a protein binding rate of over 99.9%, primarily binding to serum albumin. When used clinically to treat acne, isotretinoin is associated with a variety of adverse reactions: common skin and mucous membrane reactions include dry skin, chapped lips, dry eyes, and dry nose; some patients experience elevated blood lipid levels (total cholesterol and triglycerides) and transient increases in liver enzymes (alanine aminotransferase, ALT; aspartate aminotransferase, AST), which are usually reversible upon dose reduction or discontinuation. The most serious toxicity is teratogenicity; isotretinoin, if used in pregnant women, can cause serious birth defects (e.g., craniofacial deformities, heart defects, central nervous system malformations). [1] |
| References |
[1]. Layton A. The use of isotretinoin in acne. Dermatoendocrinol. 2009 May;1(3):162-9.
[2]. Dahl AR, et al. Inhaled isotretinoin (13-cis retinoic acid) is an effective lung cancer chemopreventive agent in A/J mice at low doses: a pilot study. Clin Cancer Res. 2000 Aug;6(8):3015-24 [3]. Bergoli RD, et al. Isotretinoin effect on alveolar repair after exodontia--a study in rats. Oral Maxillofac Surg. 2011 Jun;15(2):85-92. [4]. Ramírez-Flores PN, et al. Isotretinoin and Thalidomide Down-Regulate c-MYC Gene Expression and Modify Proteins Associated with Cancer in Hepatic Cells. Molecules. 2021 Sep 22;26(19):5742. |
| Additional Infomation |
According to an independent committee of scientific and health experts, isotretinoin may cause developmental toxicity.
cis-retinoic acid is a yellow-orange to orange crystalline powder; or an orange-brown lumpy solid. (NTP, 1992) Isotretinoin is a retinoic acid, a variant of all-trans retinoic acid in which the α,β-double bond linked to the carboxyl group is isomerized to the Z configuration. It is a synthetic retinoid drug used to treat severe acne and other skin conditions. It acts as a keratolytic agent, antitumor agent, and teratogen. It is the conjugate acid of 13-cis-retinoic acid. Isotretinoin is a retinoic acid derivative of vitamin A used to treat severe, intractable acne. It was once widely marketed under the brand name Accutane, but that brand is now discontinued. Isotretinoin poses significant risks during pregnancy and is therefore only available in the United States through the iPLEDGE program. The first product containing isotretinoin was approved by the FDA on May 7, 1982. Isotretinoin is a retinoid drug. Isotretinoin is a retinoid drug and a derivative of vitamin A, used to treat severe acne and certain types of skin cancer and head and neck cancer. Like many retinoids, isotretinoin can cause elevated serum transaminase levels, but unlike acitretin and etretinate, isotretinoin has not been definitively linked to clinically significant cases of acute liver injury with jaundice. There are reports and data regarding isotretinoin in humans. Isotretinoin is a naturally occurring retinoic acid with potential antitumor activity. Isotretinoin can bind to and activate nuclear retinoic acid receptors (RARs); activated RARs act as transcription factors, promoting cell differentiation and apoptosis. The drug also has immunomodulatory and anti-inflammatory effects and inhibits ornithine decarboxylase, thereby reducing polyamine synthesis and keratinization. It is a topical dermatological drug used to treat acne vulgaris and a variety of other skin conditions. This drug has teratogenicity and other adverse reactions. See also: Anisotretinoin (its active ingredient). Drug Indications Isotretinoin is indicated for the treatment of severe, refractory nodular acne, and in patients aged 12 years and older participating in the iPLEDGE program. FDA LabelMechanism of Action Isotretinoin works by altering cell cycle progression, cell differentiation, survival, and apoptosis. These effects reduce sebum production, preventing clogged pores and the growth of Propionibacterium acnes. Both isotretinoin and 4-oxoisotretinoin significantly reduce sebum production. Isotretinoin has low or negligible affinity for retinol-binding protein (RBP) and retinoic acid nuclear receptor (RAR). The binding of retinoic acid and 4-oxoisotretinoin to RAR-γ receptors is considered part of the mechanism of action of isotretinoin in treating acne. Isotretinoin induces sebaceous cell apoptosis, thereby reducing sebum production. Isotretinoin can also reduce hyperkeratosis through an unknown mechanism, thereby reducing acne formation. Isotretinoin does not directly kill bacteria, but it can reduce the volume of sebaceous gland ducts, creating a skin microenvironment unfavorable to the survival of Propionibacterium acnes. It may also enhance immune mechanisms and alter the chemotaxis of monocytes, thereby reducing inflammation. Preliminary evidence suggests that isotretinoin may interact with FoxO1, which may explain many of its previously unexplained effects. This review summarizes the teratogenicity of isotretinoin, focusing on species differences, toxicokinetics, and metabolism. Species insensitive to isotretinoin (rats, mice) rapidly clear the drug through detoxification, generating β-glucuronide; furthermore, placental transport in these species is limited. On the other hand, in species sensitive to isotretinoin (primates), the drug is primarily metabolized to the active metabolite 13-cis-4-oxoretinoic acid; placental transport of these metabolites is more extensive. In all tested species, placental transport of β-glucuronide was limited; these metabolites were present at extremely low concentrations in humans, sometimes undetectable. 13-cis-retinoic acid (13-retinoic acid) did not bind significantly to intracellular retinoid-binding proteins or nuclear receptors, and its tissue distribution and placental transport were also low. However, it may have extensive nucleus penetration. Due to the long half-life of 13-cis-retinoic acid, its sustained isomerization led to a significant increase in the area under the concentration-time curve (AUC) of all-trans-retinoic acid in mice, monkeys, and humans; the resulting all-trans-retinoic acid was widely distributed in the placenta and may be an important factor in the teratogenic effects of 13-cis-retinoic acid. Isomerization could not explain the teratogenic effects of 13-cis-retinoic acid in rats and rabbits. The conclusion is that isotretinoin exhibits high teratogenic activity in susceptible species (humans and monkeys), which is related to the slow elimination of the 13-cis isomer, metabolism to a 4-oxo derivative, increased placental transport, persistent isomerization, and significant exposure of target tissues to all-trans retinoic acid. Furthermore, isotretinoin lacks binding to cytoplasmic retinoid-binding proteins, which may allow it to more easily enter the cell nucleus. Isotretinoin is a first-line drug for treating moderate to severe nodular cystic acne, especially suitable for cases unresponsive to conventional treatments (e.g., topical medications, oral antibiotics). Its therapeutic mechanism includes regulating the keratinization of the follicle-sebaceous duct (reducing abnormal keratinization to prevent follicle blockage), reducing sebum secretion (inhibiting sebaceous gland activity), and exerting anti-inflammatory effects (inhibiting the activation and migration of inflammatory cells) [1] - This preliminary study suggests that low-dose inhaled isotretinoin may be a potential chemopreventive agent for lung cancer, laying the foundation for further research on its application in high-risk groups for lung cancer (such as smokers and occupationally exposed individuals) [2] - Rat studies have shown that isotretinoin can promote alveolar bone repair after tooth extraction by enhancing osteoblast function and collagen synthesis, which may have clinical significance for improving the alveolar healing prognosis of patients with poor repair ability (such as elderly patients and patients with osteoporosis). [3] Isotretinoin downregulates c-MYC gene expression in hepatocytes and modifies cancer-related proteins, indicating that it has potential anti-hepatocellular carcinoma activity, laying the foundation for further research on its role in the prevention and treatment of liver cancer. [4] |
| Molecular Formula |
C20H28O2
|
|
|---|---|---|
| Molecular Weight |
300.44
|
|
| Exact Mass |
300.208
|
|
| CAS # |
4759-48-2
|
|
| Related CAS # |
Isotretinoin-d5
|
|
| PubChem CID |
5282379
|
|
| Appearance |
Yellow crystals or reddish-orange plates from isopropyl alcohol
Yellowish to orange crystalline powder |
|
| Density |
1.0±0.1 g/cm3
|
|
| Boiling Point |
462.8±14.0 °C at 760 mmHg
|
|
| Melting Point |
172-175 °C(lit.)
|
|
| Flash Point |
350.6±11.0 °C
|
|
| Vapour Pressure |
0.0±2.5 mmHg at 25°C
|
|
| Index of Refraction |
1.556
|
|
| LogP |
6.83
|
|
| Hydrogen Bond Donor Count |
1
|
|
| Hydrogen Bond Acceptor Count |
2
|
|
| Rotatable Bond Count |
5
|
|
| Heavy Atom Count |
22
|
|
| Complexity |
567
|
|
| Defined Atom Stereocenter Count |
0
|
|
| SMILES |
CC1(C)C(/C=C/C(C)=C/C=C/C(C)=C\C(O)=O)=C(C)CCC1
|
|
| InChi Key |
SHGAZHPCJJPHSC-XFYACQKRSA-N
|
|
| InChi Code |
InChI=1S/C20H28O2/c1-15(8-6-9-16(2)14-19(21)22)11-12-18-17(3)10-7-13-20(18,4)5/h6,8-9,11-12,14H,7,10,13H2,1-5H3,(H,21,22)/b9-6+,12-11+,15-8+,16-14-
|
|
| Chemical Name |
(2Z,4E,6E,8E)-3,7-dimethyl-9-(2,6,6-trimethylcyclohex-1-en-1-yl)nona-2,4,6,8-tetraenoic acid
|
|
| Synonyms |
|
|
| HS Tariff Code |
2934.99.9001
|
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: (1). This product requires protection from light (avoid light exposure) during transportation and storage. (2). Please store this product in a sealed and protected environment (e.g. under nitrogen), avoid exposure to moisture. (3). This product is not stable in solution, please use freshly prepared working solution for optimal results. |
|
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
|
|||
|---|---|---|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.5 mg/mL (8.32 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution.
For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.08 mg/mL (6.92 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 20.8 mg/mL clear DMSO stock solution to 900 μL of corn oil and mix evenly. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 3.3285 mL | 16.6423 mL | 33.2845 mL | |
| 5 mM | 0.6657 mL | 3.3285 mL | 6.6569 mL | |
| 10 mM | 0.3328 mL | 1.6642 mL | 3.3285 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
| NCT Number | Recruitment | interventions | Conditions | Sponsor/Collaborators | Start Date | Phases |
| NCT04660916 | Completed | Drug: Isotretinoin | Isotretinoin Nail Abnormality |
Sinan Özçelik | October 22, 2019 | |
| NCT06225570 | Not yet recruiting | Drug: Isotretinoin Drug: Tetracycline |
Acne Vulgaris | Medical University of South Carolina | February 2024 | Early Phase 1 |
| NCT04204304 | Completed | Drug: Isotretinoin | Isotretinoin Adverse Reaction Vitamin D Deficiency |
Ankara Training and Research Hospital | March 15, 2019 | Not Applicable |
| NCT05218486 | Active, not recruiting | Drug: Isotretinoin | Acne Vulgaris | Alshimaa Abbas Mohamed Ebrahim | August 1, 2021 | Phase 4 |
|
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved





























 NMR
NMR