| Size | Price | Stock | Qty |
|---|---|---|---|
| 10mg |
|
||
| 25mg |
|
||
| 50mg |
|
||
| 100mg |
|
||
| 250mg |
|
||
| 500mg | |||
| Other Sizes |
Purity: ≥98%
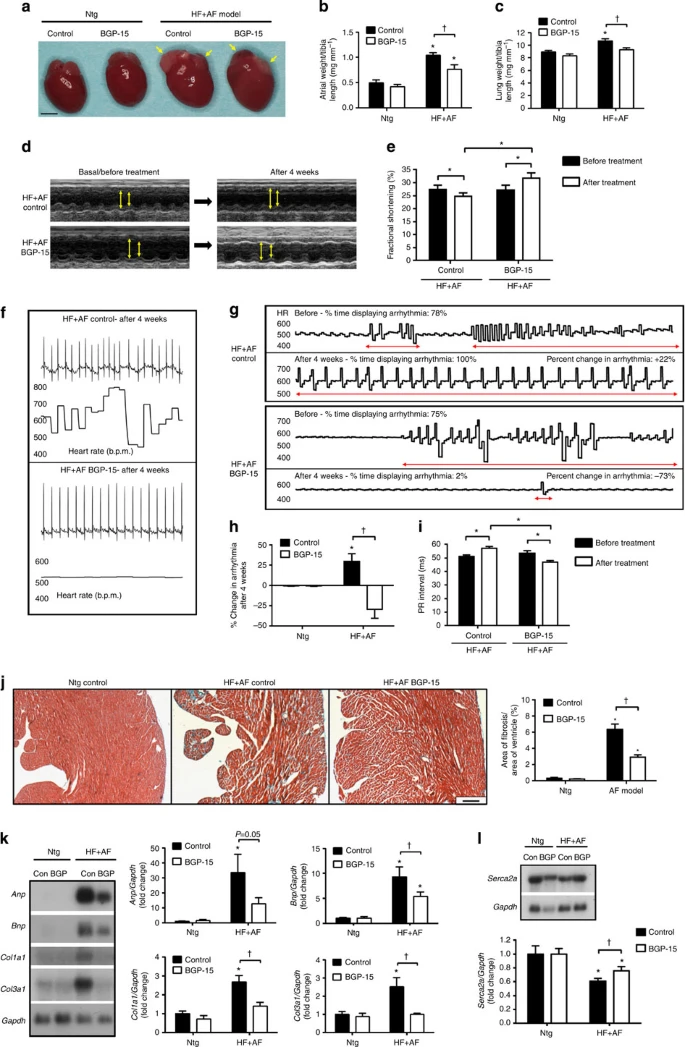
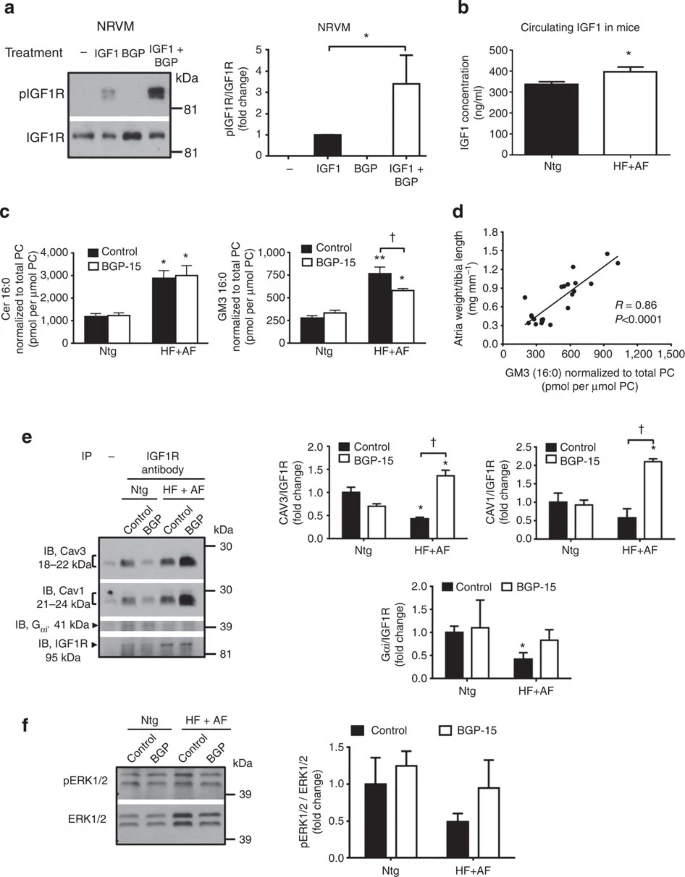
BGP-15 HCl is a potent and novel PARP inhibitor that can protect against heart failure and atrial fibrillation in mice. At 200 μM, BGP-15 inhibits the oxidative damage caused by imatinib mesylate, reduces the loss of high-energy phosphates, modifies the signaling effect of imatinib mesylate by blocking p38 MAP kinase and JNK activation, and stimulates Akt and GSK-3beta phosphorylation. An in-vivo investigation revealed that in two mouse models of HF and AF, BGP-15 enhanced cardiac function and decreased arrhythmic episodes. BGP-15 was linked to higher IGF1R phosphorylation in these models.
| Targets |
PARP (IC50 =120 μM)
|
|---|---|
| ln Vitro |
At 200 μM, BGP-15 inhibits the oxidative damage caused by imatinib mesylate, stops the consumption of high-energy phosphates, and modifies the signaling effects of imatinib mesylate by inhibiting p38 MAP damage, JNK activation, and Sensing Akt and GSK-3beta[5].
|
| ln Vivo |
In old mdx mice, BGP-15 (15 mg/kg, cervical) had no effect on skeletal muscle pathology [1]. Although it did not stop diaphragm muscle atrophy, 10 days of BGP-15 therapy significantly increased diaphragm muscle fiber function in the stent model (about 100%). Additionally, by preventing myosin PTM linked to PARP-1 suppression and HSP72 activation, this therapy enhances septal content and function [2]. The effects of BGP-15 (15 mg/kg daily in saline) were assessed using morphological, cardiac function, and electrocardiographic measures in independent cohorts of Ntg mice or normal wild-type mice. Treatment with BGP-15 decreased the growth in lung weight and atrial size. Arrhythmias can be prevented or their consequences lessened with BGP-15 medication. In the HF+AF paradigm, BGP-15 processing is linked to the PR interval [3]. In pillow-fed rabbits, BGP-15 (10 and 30 mg/kg) raised polenta by 50% and 70%, respectively, but not in normal rabbits. Following a 5-day course of therapy with BGP-15, the rate of mutation infusion enhanced in hereditary insulin-resistant GK in a dose-dependent way. When compared to carbon dioxide, the most effective dose is 20 mg/kg, which increases insulin load by 71% [4].
|
| Enzyme Assay |
The protective effect of O-(3-piperidino-2-hydroxy-1-propyl)nicotinic amidoxime (BGP-15) against ischemia-reperfusion-induced injury was studied in the Langendorff heart perfusion system. To understand the molecular mechanism of the cardioprotection, the effect of BGP-15 on ischemic-reperfusion-induced reactive oxygen species (ROS) formation, lipid peroxidation single-strand DNA break formation, NAD(+) catabolism, and endogenous ADP-ribosylation reactions were investigated. These studies showed that BGP-15 significantly decreased leakage of lactate dehydrogenase, creatine kinase, and aspartate aminotransferase in reperfused hearts, and reduced the rate of NAD(+) catabolism. In addition, BGP-15 dramatically decreased the ischemia-reperfusion-induced self-ADP-ribosylation of nuclear poly(ADP-ribose) polymerase(PARP) and the mono-ADP-ribosylation of an endoplasmic reticulum chaperone GRP78. These data raise the possibility that BGP-15 may have a direct inhibitory effect on PARP. This hypothesis was tested on isolated enzyme, and kinetic analysis showed a mixed-type (noncompetitive) inhibition with a K(i) = 57 +/- 6 microM. Furthermore, BGP-15 decreased levels of ROS, lipid peroxidation, and single-strand DNA breaks in reperfused hearts. These data suggest that PARP may be an important molecular target of BGP-15 and that BGP-15 decreases ROS levels and cell injury during ischemia-reperfusion in the heart by inhibiting PARP activity [6].
|
| Cell Assay |
In this study, researchers investigate the cardiotoxic effects of the well-known cytostatic agent imatinib mesylate (Gleevec), and presented evidence for the cardioprotective effect of BGP-15 which is a novel insulin sensitizer. The cardiotoxic effect of imatinib mesylate was assessed in Langendorff rat heart perfusion system. The cardiac high-energy phosphate levels (creatine phosphate (PCr) and ATP) were monitored in situ by (31)P NMR spectroscopy. The protein oxidation, lipid peroxidation, and the activation of signaling pathways were determined from the freeze-clamped hearts. Prolonged treatment of the heart with imatinib mesylate (20 mg/kg) resulted in cardiotoxicity, which were characterized by the depletion of high-energy phosphates (PCr and ATP), and significantly increased protein oxidation and lipid peroxidation. Imatinib mesylate treatment-induced activation of MAP kinases (including ERK1/2, p38, and JNK) and the phosphorylation of Akt and GSK-3beta. BGP-15 (200 μM) prevented the imatinib mesylate-induced oxidative damages, attenuated the depletion of high-energy phosphates, altered the signaling effect of imatinib mesylate by preventing p38 MAP kinase and JNK activation, and induced the phosphorylation of Akt and GSK-3beta. The suppressive effect of BGP-15 on p38 and JNK activation could be significant because these kinases contribute to the cell death and inflammation in the isolated perfused heart.[5]
|
| Animal Protocol |
Male adult HF+AF and Ntg mice, who are approximately 4 months old, are given BGP-15 (15 mg/kg daily in saline) or left untreated (oral gavage with saline or no gavage) for 4 weeks. In the HF+AF model, gavage with saline has no effect on morphological or functional parameters. Thus, mice receiving saline injection and mice left untreated (no gavage) are grouped together and referred to as HF+AF control. ECG and echocardiography scans are carried out both before and after therapy.
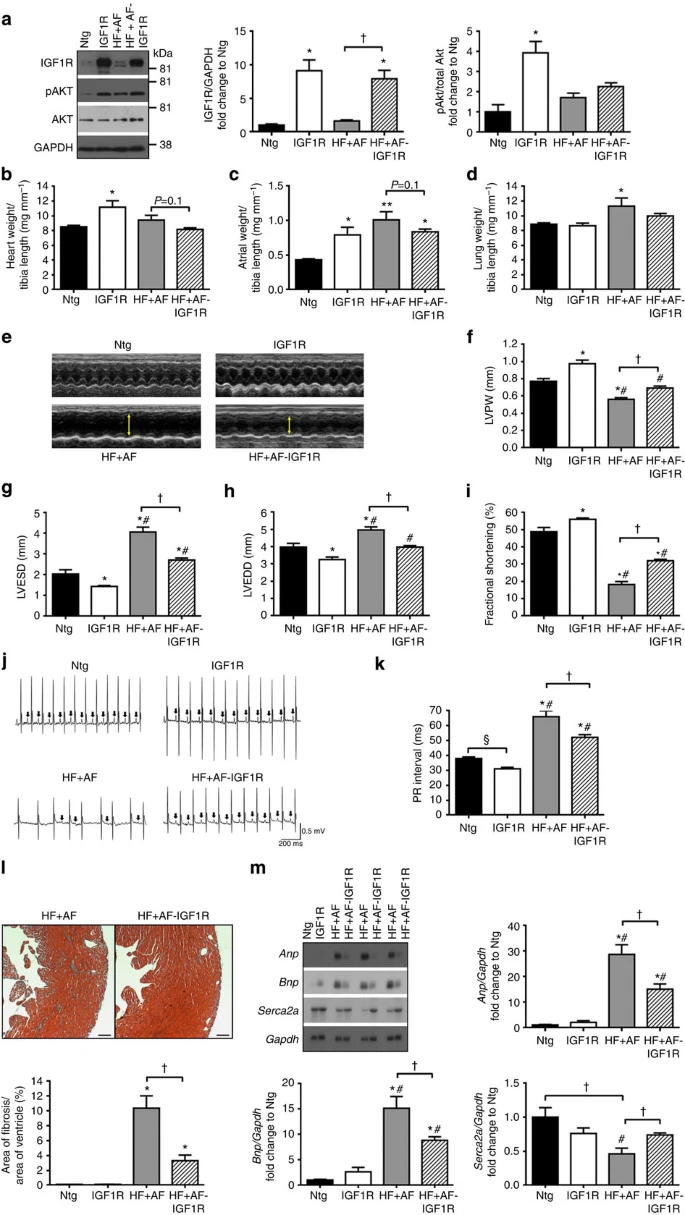
Experimental protocols[3] Protocol 1: Adult (~4 month) male HF+AF and Ntg mice were administered with BGP-15 (15 mg kg−1 per day in saline, N-Gene Research Laboratories) for 4 weeks by oral gavage or remained untreated (oral gavage with saline or no gavage). Gavage with saline had no effect on morphological or functional parameters in the HF+AF model (Supplementary Fig. 3). Therefore, untreated mice (no gavage) and mice administered saline are combined and referred to as HF+AF control. Echocardiography and ECG studies were performed before and after treatment.[3] Protocol 2: To determine whether BGP-15 provided protection via HSP70, BGP-15 (15 mg kg−1 per day, oral gavage) was administered to adult (~14 weeks) male and female HF+AF mice deficient for HSP70 (HF+AF-HSP70 KO) for 4 weeks.[3] Protocol 3: To assess whether an increase in HSP70 could mediate protection in the HF+AF model, male HF+AF mice overexpressing HSP70 (HF+AF-HSP70 Tg) were generated and characterized at ~12–13 weeks.[3] Protocol 4: To examine whether overexpression of IGF1R in the heart could provide protection in the HF+AF model, male HF+AF mice overexpressing IGF1R (HF+AF-IGF1R Tg) were generated and characterized at ~16–17 weeks.[3] Protocol 5: To determine whether IGF1R could mediate protection in the HF+AF model independent of HSP70, male and female HF+AF-IGF1R Tg-HSP70 KO mice were generated and characterized at ~11 weeks.[3] Protocol 6: To examine whether BGP-15 had the capacity to provide protection in an additional model with HF and AF, 11- to 12-month-old male MURC Tg were administered with BGP-15 (15 mg kg−1 per day, oral gavage) or saline for 4 weeks.[3] To assess whether BGP-15 administration could confer effects on an already established dystrophic pathology, 20-week-old mdx and 8-week-old dko mice were administered BGP-15 (15 mg/kg in 0.9% sterile saline; N-Gene Research Laboratories Inc., New York, NY) daily via oral gavage for 4 (dko) or 5 (mdx) weeks. Age-matched vehicle-treated dystrophic and healthy wild-type control (C57BL/10) mice received an equivalent volume of 0.9% sterile saline via daily oral gavage. Because of the severity of the dko phenotype, a shorter treatment period was used with a significant number of mice reaching humane end point criteria (ie, kyphosis score of 5 and sustained 15% loss of body mass) after 12 weeks of age. The average lifespan of mice in our dko colony was approximately 14 to 15 weeks, with the severity of the dystrophic pathology at 8 weeks of age (when treatment commenced) indicated by an average kyphosis score of 2.5. The kyphosis score indicates the severity of spinal curvature on palpation of conscious mice and ranked 1 to 5, with 1 indicating no spinal deformity and 5 being the most severe. To assess the effect of BGP-15 administration as a preventive treatment for the dystrophic cardiomyopathy and to confirm previous findings on skeletal muscles of young mice,14 4-week-old dko mice were administered BGP-15 (15 mg/kg in 0.9% sterile saline daily via oral gavage) for 5 to 6 weeks, with other groups of aged-matched dko and C57BL/10 mice treated similarly with vehicle only. Because BGP-15 is a hydroxylamine derivative that affects only stressed cells, a group of C57BL/10 mice treated with BGP-15 was not included.10,14,34 Previous studies investigating BGP-15 effects on skeletal muscle and heart observed no morphological or functional changes in either tissue, in wild-type mice after long-term treatment.14,34 To assess Hsp72 induction via BGP-15, 4- and 10-week-old dko mice and age-matched C57BL/10 mice were administered a single bolus of BGP-15 (15 mg/kg) via oral gavage, and the tibialis anterior (TA) muscles, heart, and diaphragm were excised 6 hours later, frozen in liquid nitrogen, and stored at −80°C for later analyses.[1] |
| References |
|
| Additional Infomation |
Duchenne muscular dystrophy is a severe, progressive rhabdomyotrophic disorder that leads to respiratory and/or heart failure, ultimately resulting in premature death. We previously demonstrated that treatment with the heat shock protein 72 co-inducer BGP-15 in young malnourished MDX mice and dystrophin/myotrophic knockout (dko) mice improved their malnutrition pathology. Therefore, we hypothesized that late-stage BGP-15 treatment in older MDX and DKO mice would be equally effective given established malnutrition pathology. However, late-stage BGP-15 treatment in either MDX or DKO mice did not improve the maximum contractile force of the tibialis anterior (TA) (in vivo) or the diaphragmatic strip (in vitro). However, collagen deposition (fibrosis) was reduced in the tibialis anterior (TA) of BGP-15-treated DKO mice, but not in the TA of treated MDX mice or the diaphragm of treated MDX and DKO mice. We also investigated whether BGP-15 treatment could improve certain aspects of cardiac pathology, and the results showed that in young dko mice, BGP-15 treatment reduced collagen deposition and improved cell membrane integrity and contractile function. These results confirm that BGP-15 can improve certain aspects of malnutrition pathology, but its efficacy on the heart and skeletal muscle varies at different stages of disease progression. These findings support the role of BGP-15 in a range of pharmacological treatments for Duchenne muscular dystrophy and related diseases. [1]
Ventilation-induced diaphragmatic dysfunction (VIDD) refers to a significant decline in diaphragmatic function after mechanical ventilation, which has a negative impact on patients’ quality of life and the healthcare system, but there is currently a lack of targeted treatment strategies. We used an experimental intensive care unit (ICU) model to conduct time-resolved studies on changes in diaphragmatic structure and function caused by long-term mechanical ventilation and the effects of pharmacological intervention (the molecular chaperone co-inducer BGP-15). The significant loss of diaphragmatic fiber function caused by mechanical ventilation is caused by post-translational modification (PTM) of myosin. In rat models, diaphragmatic fiber function was significantly improved (approximately 100%) after 10 days of BGP-15 treatment, but diaphragmatic atrophy was not reversed. The treatment also protected the diaphragm from the effects of myosin PTM associated with HSP72 induction and PARP-1 inhibition, thereby improving mitochondrial function and content. Therefore, BGP-15 may provide an intervention strategy for reducing ventilator-associated diaphragmatic dysfunction (VIDD) in mechanically ventilated ICU patients. [2] Heart failure (HF) and atrial fibrillation (AF) share common risk factors, often occur together, and have high mortality rates. Treatment of heart failure (HF) with atrial fibrillation remains a major unsolved problem. This study showed that the small molecule BGP-15 improved cardiac function and reduced the occurrence of arrhythmias in two independent mouse models that gradually developed heart failure and atrial fibrillation. In these models, BGP-15 treatment was associated with increased phosphorylation of insulin-like growth factor 1 receptor (IGF1R), while phosphorylation of IGF1R was significantly reduced in atrial tissue samples from patients with atrial fibrillation. Overexpression of the heart-specific IGF1R transgene in mice with heart failure and atrial fibrillation reproduced the protective effect observed with BGP-15. We further confirmed that BGP-15 and IGF1R provide protection independent of phosphatidylinositol 3-kinase-Akt and heat shock protein 70, which are often deficient in aging and diseased hearts. Given that BGP-15 is safe and well-tolerated in humans, this study reveals a potential approach for treating heart failure and atrial fibrillation. [3] Background: Insulin resistance has been considered the most important predictor of the further development of type 2 diabetes mellitus (T2DM). This study investigated the effect of the heat shock protein (HSP) co-inducer BGP-15 on insulin sensitivity in different insulin-resistant animal models and compared it with insulin secretagogues and insulin sensitizers. Methods: Insulin sensitivity in normal rabbits, high-cholesterol-fed rabbits, and healthy Wistar and Goto-Kakizaki (GK) rats was assessed using the high-insulin positive glucose clamp technique, and dose range studies were conducted. We also investigated the effect of BGP-15 on streptozotocin-induced aortic vasodilation in Sprague-Dawley rats. Results: In cholesterol-fed rabbits, BGP-15 at doses of 10 mg/kg and 30 mg/kg increased insulin sensitivity by 50% and 70%, respectively, but this was not observed in normal rabbits. In GK rats with hereditary insulin resistance, glucose infusion rate increased in a dose-dependent manner after 5 days of BGP-15 treatment. The most effective dose was 20 mg/kg, which increased insulin sensitivity by 71% compared to the control group. Administration of BGP-15 protected blood vessels from streptozotocin-induced changes, with effects similar to rosiglitazone. Conclusion: Our results indicate that the insulin-sensitizing effect of BGP-15 is comparable to that of conventional insulin sensitizers. This may have clinical value for the treatment of type 2 diabetes. [4] |
| Molecular Formula |
C14H24CL2N4O2
|
|---|---|
| Molecular Weight |
351.27
|
| Exact Mass |
350.128
|
| Elemental Analysis |
C, 47.87; H, 6.89; Cl, 20.19; N, 15.95; O, 9.11
|
| CAS # |
66611-37-8
|
| Related CAS # |
66611-38-9; 66611-37-8 (HCl)
|
| PubChem CID |
9884807
|
| Appearance |
White solid powder
|
| LogP |
2.807
|
| Hydrogen Bond Donor Count |
4
|
| Hydrogen Bond Acceptor Count |
5
|
| Rotatable Bond Count |
6
|
| Heavy Atom Count |
22
|
| Complexity |
306
|
| Defined Atom Stereocenter Count |
0
|
| SMILES |
Cl[H].Cl[H].O([H])C([H])(C([H])([H])O/N=C(/C1=C([H])N=C([H])C([H])=C1[H])\N([H])[H])C([H])([H])N1C([H])([H])C([H])([H])C([H])([H])C([H])([H])C1([H])[H]
|
| InChi Key |
ISGGVCWFTPTHIX-UHFFFAOYSA-N
|
| InChi Code |
InChI=1S/C14H22N4O2.2ClH/c15-14(12-5-4-6-16-9-12)17-20-11-13(19)10-18-7-2-1-3-8-18;;/h4-6,9,13,19H,1-3,7-8,10-11H2,(H2,15,17);2*1H
|
| Chemical Name |
N'-(2-hydroxy-3-piperidin-1-ylpropoxy)pyridine-3-carboximidamide;dihydrochloride
|
| Synonyms |
BGP15 hydrochloride; BGP15 HCl; BGP15; N-(2-Hydroxy-3-(piperidin-1-yl)propoxy)nicotinimidamide dihydrochloride; 3-Pyridinecarboximidamide, N-(2-hydroxy-3-(1-piperidinyl)propoxy)-, hydrochloride (1:2); RLN2GTG4YS; N'-(2-hydroxy-3-piperidin-1-ylpropoxy)pyridine-3-carboximidamide;dihydrochloride; 3-Pyridinecarboximidamide, N-(2-hydroxy-3-(1-piperidinyl)propoxy)-, dihydrochloride; BGP 15; BGP-15
|
| HS Tariff Code |
2934.99.9001
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: Please store this product in a sealed and protected environment, avoid exposure to moisture. |
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
H2O : ~100 mg/mL (~284.68 mM)
DMSO : ~11.33 mg/mL (~32.25 mM) |
|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.5 mg/mL (7.12 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution.
For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.5 mg/mL (7.12 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. View More
Solubility in Formulation 3: ≥ 2.5 mg/mL (7.12 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. Solubility in Formulation 4: 100 mg/mL (284.68 mM) in PBS (add these co-solvents sequentially from left to right, and one by one), clear solution; with ultrasonication. |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 2.8468 mL | 14.2341 mL | 28.4681 mL | |
| 5 mM | 0.5694 mL | 2.8468 mL | 5.6936 mL | |
| 10 mM | 0.2847 mL | 1.4234 mL | 2.8468 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
|
|
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved





























































 COA
COA