| Size | Price | Stock | Qty |
|---|---|---|---|
| 5g |
|
||
| 10g |
|
||
| 25g |
|
||
| 50g |
|
||
| 100g | |||
| Other Sizes |
































Purity: ≥98%
Amantadine HCl (EXP-105-1; GP 38026; ADS5102; Influenol; Midantan; Midantane; Mydantane; NSC 83653; Symadine; Symmetrel; Trivaline; Virasol; Viregyt; Virofral; Virosol), the hydrochloride salt of amantadine, is an approved medication used to treat or prevent infections of the respiratory tract caused by a certain virus. Amantadine has been approved by the FDA to be used as an antiviral and an antiparkinsonian medication.
| Targets |
Influenza A viruses; ion channels NMDA, M2; CDK2; Bcl-2; Bax
|
|---|---|
| ln Vitro |
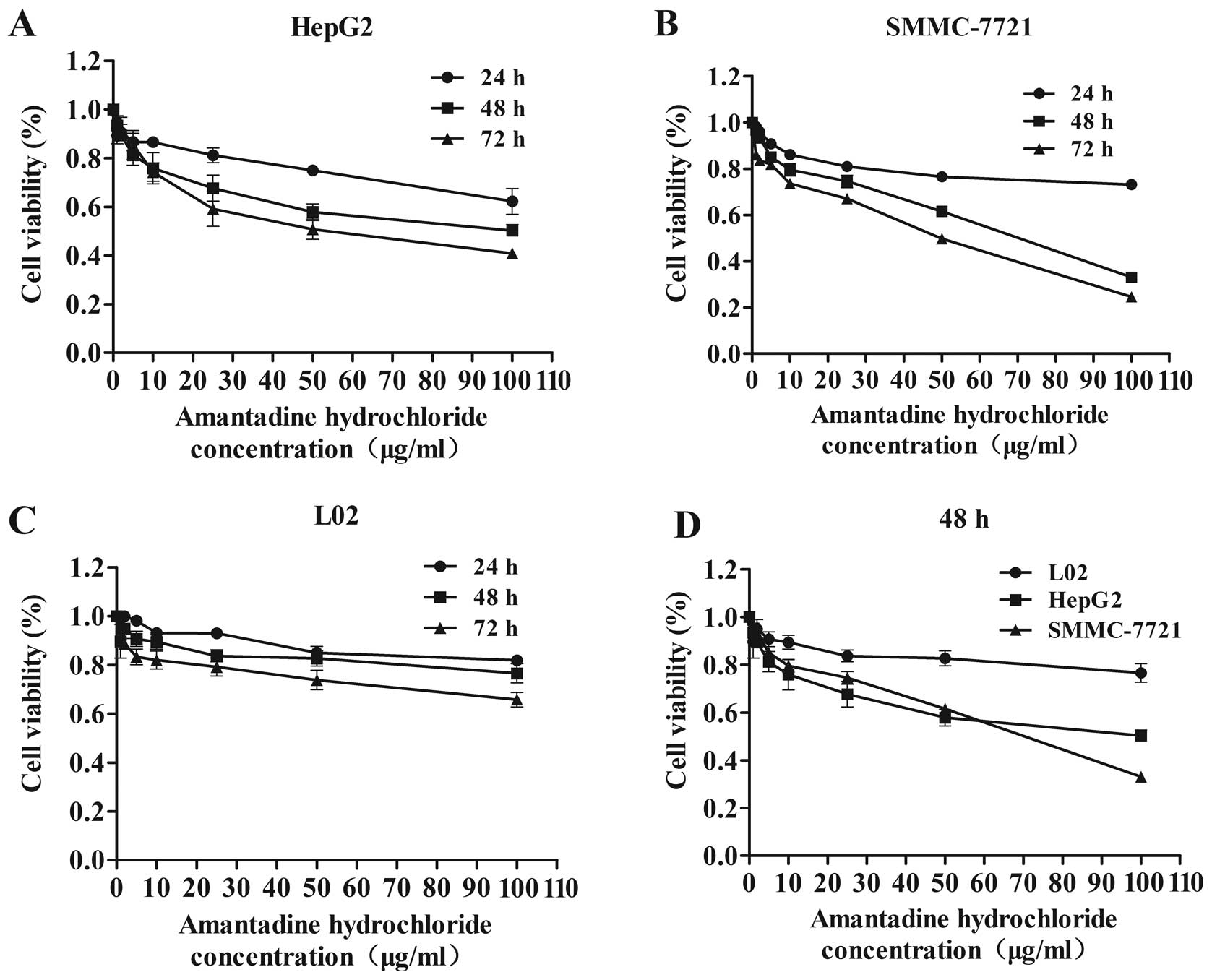
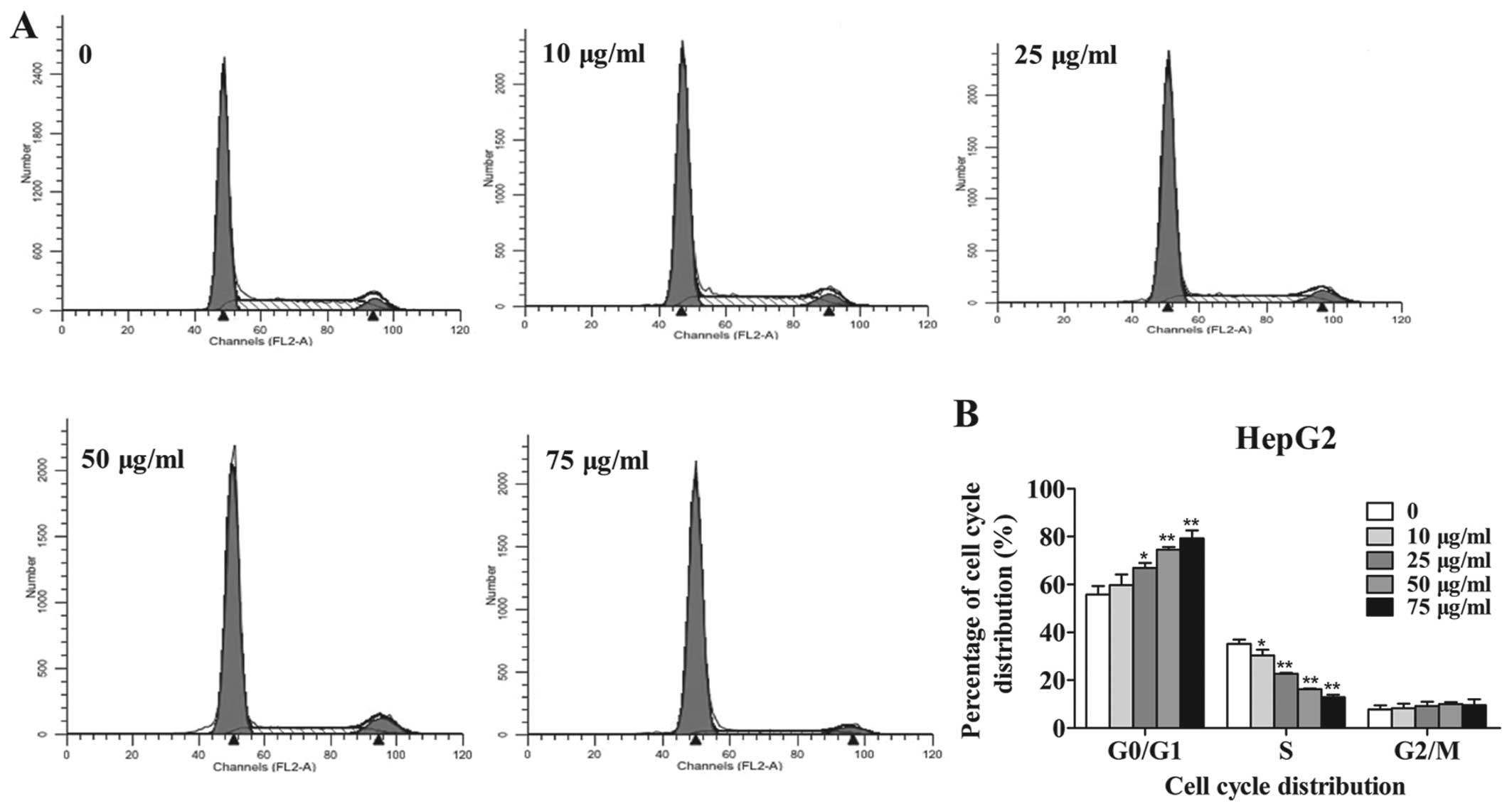
Amantadine hydrochloride (0-500 μM, 26 hours) inhibits SARS-CoV-2 replication with IC50 concentrations between 83 and 119 μM [4]. Amantadine hydrochloride (0-100 μg/mL, 24-72 h) significantly inhibits HepG2. Amantadine hydrochloride (0-75 μg/mL, 48 h) blocks the cell cycle in the G0/G1 phase and induces cell swelling [6]. Amantadine hydrochloride (0-75 μg) and swelling of SMMC-7721 cells [6]. /mL, 48 h) can reduce cell cycle-related genes and proteins (cyclin D1, cyclin E and CDK2), reduce Bcl-2 and increase Bax protein and mRNA levels [6]. Cell Viability Assay[4] Cell Line: Vero E6 Cell Concentration: 500 µM, 100 µM, 20 µM, 4 µM and 8 nM Incubation time: 26 hours Results: Concentration of viral nucleic acid in the supernatant after 26 hours of infection at 10°C Reduced dependence (IC50=83 µM) -500 µM. Results in a concentration-dependent reduction of viral nucleic acid in the cytoplasm (IC50=119 µM) 26 hours post-infection. Cell proliferation assay[6] Cell lines: Human HCC cell lines (HepG2 and SMMC-7721) and normal liver cells (L02 cells) Concentrations: 0, 1, 2, 5, 10, 25, 50 and 100 µg/mL Incubation time : 24, 48 and 72 hours Results: Inhibited cell proliferation in a time- and dose-dependent manner in HepG2 and SMMC-7721 cells. Cell cycle analysis[6] Cell lines: HepG2 and SMMC-7721 Cell concentrations: 0, 10, 25, 50 and 75 µg/mL Incubation time: 48 hours Results: Significant increase in the number of HepG2 and SMMC-7721 cells in G0/G1 phase in a dose-dependent manner, and significantly reduced the number of HepG2 cells in the S phase. Apoptosis analysis[6] Cell lines: HepG2 and SMMC-7721 Cell concentrations: 0, 10, 25, 50 and 75 µg/mL Incubation time: 48 hours Results: Significant increase in the percentage of apoptotic HepG2 and SMMC-7721 cells (early- and late-stage apoptosis) in a dose-dependent manner. Western Blot Analysis[6] Cell lines: HepG2 and SMMC-7721 Cell concentrations: 0, 10, 25, 50 and 75 µg/mL Incubation time: 48 h Results: showed downregulation of cyclin D1, cyclin E and CDK2, and showed that HepG2 and Bcl-2 levels were reduced and Bax levels were increased in SMMC-7721 cells. RT-PCR[6] Cell lines: HepG2 and SMMC-7721 Cell concentrations: 0, 10, 25, 50 and 75 µg/mL Incubation time: 48 hours Results: Showed an increase in Bax and a decrease in Bcl-2 gene.
The suppression of SARS-CoV-2 replication by amantadine (0-500 µM, 26 hours) ranges in IC50 values from 83 to 119 µM [4]. Amantadine (0-100 µg/mL, 24-72 hours) strongly suppresses HepG2 and SMMC-7721 cell growth [6]. Amantadine (0-75 µg/mL, 48 hours) causes apoptosis and stops the cell cycle in the G0/G1 phase [6]. Amantadine (0-75 µg/mL, 48 hours) decreases Bcl-2, increases Bax protein and mRNA levels, and decreases cell cycle-related genes and proteins (cyclin D1, cyclin E, and CDK2) [6]. Since the SARS-CoV-2 pandemic started in late 2019, the search for protective vaccines and for drug treatments has become mandatory to fight the global health emergency. Travel restrictions, social distancing, and face masks are suitable counter measures, but may not bring the pandemic under control because people will inadvertently or at a certain degree of restriction severity or duration become incompliant with the regulations. Even if vaccines are approved, the need for antiviral agents against SARS-CoV-2 will persist. However, unequivocal evidence for efficacy against SARS-CoV-2 has not been demonstrated for any of the repurposed antiviral drugs so far. Amantadine was approved as an antiviral drug against influenza A, and antiviral activity against SARS-CoV-2 has been reasoned by analogy but without data. We tested the efficacy of Amantadine in vitro in Vero E6 cells infected with SARS-CoV-2. Indeed, amantadine inhibited SARS-CoV-2 replication in two separate experiments with IC50 concentrations between 83 and 119 µM. Although these IC50 concentrations are above therapeutic amantadine levels after systemic administration, topical administration by inhalation or intranasal instillation may result in sufficient amantadine concentration in the airway epithelium without high systemic exposure. However, further studies in other models are needed to prove this hypothesis.[4] Hepatocellular carcinoma (HCC) is one of the most aggressive malignancies worldwide, and its incidence associated with viral infection has increased in recent years. Amantadine is a tricyclic symmetric amine that can effectively protect against the hepatitis C virus. However, its antitumor properties remain unclear. In the present study, the effects of Amantadine on tumor cell viability, cell cycle regulation and apoptosis were investigated. The growth of HepG2 and SMMC‑7721 cells (HCC cell lines) was detected by an MTT assay. Flow cytometry was used to investigate cell cycle regulation and apoptosis. Reverse transcription‑quantitative polymerase chain reaction and western blot analysis were also performed to examine the expression of cell cycle‑ and apoptosis‑related genes and proteins, including cyclin E, cyclin D1, cyclin‑dependent kinase 2 (CDK2), B‑cell lymphoma 2 (Bcl‑2) and Bax. Our results demonstrated that amantadine markedly inhibited the proliferation of HepG2 and SMMC‑7721 cells in a dose‑ and time‑dependent manner and arrested the cell cycle at the G0/G1 phase. The levels of the cell cycle‑related genes and proteins (cyclin D1, cyclin E and CDK2) were reduced by amantadine, and apoptosis was significantly induced. Amantadine treatment also reduced Bcl‑2 and increased the Bax protein and mRNA levels. Additionally, Bcl‑2/Bax ratios were lower in the two HCC cell lines following amantadine treatment. Collectively, these results emphasize the role of amantadine in suppressing proliferation and inducing apoptosis in HCC cells, advocating its use as a novel tumor-suppressive therapeutic candidate [6]. |
| ln Vivo |
Amantadine hydrochloride (25 mg/kg, IP, once daily for 3 days) inhibits neuromodulation and learning and memory impairments caused by conditioning [5]. Animal model: Fischer 344 rats (4 months old, male, 290-330 g, 15 rats per group) [5] Dosage: 25 mg/kg Administration method: IP, once daily for 3 consecutive days (surgery 15 minutes before the first administration) Results: Inhibition of neuroinflammation and learning and memory impairment caused by surgery, increased GDNF (glial cell line-derived neurotrophic factor) and glial fibrillary acidic protein (star) in the hippocampus morphocyte markers) colocalized.
Amantadine (25 mg/kg, IP, once day for 3 days) reduces surgery-induced neuroinflammation and learning and memory deficits [5]. Surgery increased the time to identify the target box in the Barnes maze when tested 1 day [22 (median) (11-66) (interquartile range) of control group vs. 158 (29-180) of surgery group, n = 15, P = 0.022) or 8 days after the training sessions and reduced context-related freezing behavior in the fear conditioning test. These effects were attenuated by Amantadine (25 (14-90), n = 15, P = 0.029 compared with surgery group at 1 day after the training sessions in Barnes maze) and intracerebroventricular GDNF. Amantadine increased GDNF that was co-localized with glial fibrillary acidic protein, an astrocytic marker, in the hippocampus. Intracerebroventricular injection of an anti-GDNF antibody but not the denatured antibody blocked the effects of amantadine on cognition. Surgery induced neuroinflammation that was inhibited by amantadine. Lipopolysaccharide increased interleukin 1β production from C8-B4 cells. This effect was inhibited by GDNF [5]. Amantadine attenuated surgery-induced learning and memory impairment [5] The time to identify the target box during the 4-day training sessions of Barnes maze test was reduced with increased training sessions in the control rats, rats received anesthesia only, rats received amantadine only and rats received surgery plus Amantadine. This time on day 4 was significantly shorter than that on day 1 for these four groups of rats. This effect was not apparent in the rats after surgery alone. Surgery had a significant effect on the time needed to identify the target box in the training sessions [F(1,28) = 5.625, P = 0.025]. This effect was abolished by amantadine [F(1,28) = 0.840, P = 0.367; compared with control group]. Amantadine or anesthesia only did not have a significant effect on the time to identify the target box during the training sessions [F(1,28) = 0.063, P = 0.804; F(1, 14) = 0.074, P + 0.790] (Figs. 1 and 2). When the rats were tested 1 day after the training sessions, the time to identify the target box for the rats subjected to surgery was longer than that for the control rats. This prolongation was attenuated by amantadine. A similar change pattern occurred when the test was performed 8 days after the training sessions. However, anesthesia and amantadine alone did not affect the time to identify the target box whether the test was performed 1 day or 8 days after the training sessions (Fig. 1B and 2B). Rats in the surgery group but not in the anesthesia only group or amantadine group had less context-related freezing behavior in the fear conditioning test than control rats. This surgical effect was abolished by amantadine (Fig. 1C). There was no difference in the tone-related freezing behavior among the control rats, rats received amantadine, rats received surgery and rats received surgery plus amantadine (Fig. 1C and 2C). Amantadine attenuated surgery-induced neuroinflammation [5] The expression of Iba-1 (a microglial marker), IL-1β and IL-6 in the hippocampus was significantly increased at 6 and 24 h after the surgery. These increases were abolished by amantadine (Figs. 3 and 4). Similarly, Iba-1 expression in the hippocampal dentate gyrus region was also increased at 10 days after the surgery and this increase was blocked by Amantadine (Fig. 5). These results suggest that surgery induces neuroinflammation that was inhibited by amantadine. Amantadine increased the expression of GDNF that inhibited microglial activation [5] Amantadine significantly increased GDNF in the hippocampus (Fig. 7). GDNF was mainly co-localized with GFAP, an astrocytic marker, but was not co-localized with Iba-1 (Figs. 7A and 7B). Some GDNF appeared to be around NeuN, a neuronal marker (Fig. 7C). Surgery also increased GFAP but this increase was not affected by Amantadine in the hippocampus (Figs. 7A and 7E). Amantadine-induced attenuation of learning and memory impairment after surgery was inhibited by anti-GDNF antibody [5] Similar to the control rats, rats in antibody only group and the surgery plus Amantadine plus boiled antibody group had a decreased time to find the target box with increased training sessions. This time on the training day 4 was shorter than that on training day 1 for these two groups of rats. This effect was not apparent for rats in the surgery plus amantadine plus anti-GDNF antibody group. The anti-GDNF antibody was found to have a significant effect on the time to identify the target box during the training sessions [F(1,14) = 19.009, P < 0.001; compared with control) (Fig. 9A). The time to identify the target box on day 1 after the training session was not different among control rats, rats received antibody, rates received surgery plus amantadine plus anti-GDNF antibody or rats received surgery plus amantadine plus boiled antibody. However, rats subjected to surgery plus amantadine plus anti-GDNF antibody required much longer time than control rats or rats received surgery plus amantadine plus boiled antibody to identify the target box on day 8 after the training sessions (Fig. 9B). Similarly, rats subjected to surgery plus amantadine plus anti-GDNF antibody also had less context-related freezing behavior than control rats or rats received surgery plus amantadine plus boiled antibody in the fear conditioning test. However, the tone-related freezing behavior was not different among the three groups (Fig. 9C). |
| Enzyme Assay |
S-Protein—ACE2 Binding Assay [4]
The compounds were tested for their ability to inhibit the binding of SARS-CoV-2 spike protein (S protein) to ACE2 using the SARS-CoV-2 spike: ACE2 Inhibitor Screening Assay Kit. In brief, the SARS-CoV-2 spike protein was coated to a 96 microwell plate at 1 µg/mL in phosphate buffered saline. Unbound protein was removed and unspecific binding sites in the wells are blocked. Then, the blocking solution was removed, and the diluted compounds and control samples were added to the wells. After pre-incubation of the coated spike protein with the compounds, the His-tagged ACE2 protein was added and incubated together with the compounds to allow binding to the spike protein. After washing and blocking, the bound ACE2 protein was detected by an anti-His-antibody coupled to horse radish peroxidase (HRP). The detection was performed using a chemiluminescent HRP substrate and reading the luminescence intensity in a microtiter-plate reader. The luminescence signal of each sample containing diluted compound was divided by the luminescence in absence of any inhibitor, and the resulting values were plotted against the concentration of the compound. Antiviral Activity Assay with RT-PCR Readout (1st Experiment) [4] Exponentially growing Vero E6 cells were seeded into a 48-well plate at a density of 8 × 104 cells per well and were incubated overnight. Medium was removed and cells were infected in triplicate with SARS-CoV-2 (hCoV-19/Italy/INMI1-isl/2020 at an MOI of 0.01 in 300 µL of medium containing different inhibitor concentrations. Amantadine was solubilized in sterile water and further diluted with medium to concentrations of 500 µM, 100 µM, 20 µM, 4 µM, and 8 nM. Remdesivir was solubilized in DMSO and diluted with medium to concentrations of 50 µM, 10 µM, 2 µM, 0.4 µM, and 80 nM. Remdesivir MOCK control contained according amounts of DMSO. Antiviral Activity Assay with Nucleocapsid Protein Readout (2nd Experiment) [4] Exponentially growing Vero E6 cells were seeded into a 96-well plate at their optimal density in complete medium; 24 h later, cells were infected with SARS-CoV-2 (viral strain INMI1) at 0.01 moi (multiplicity of infection) and then exposed to different concentrations of the drugs (0–0.1–1–10–100–300 μM for Amantadine for 72 h. Drug dilutions were performed in culture medium. Replicates for each concentration point were examined. At the end of the incubation period, antiviral activity was examined through both ELISA (quantifying SARS-CoV-2 nucleoprotein) as well as a cytoprotection assay (toxicity effect examined through an inverted microscope). |
| Cell Assay |
Cell Viability Assay[4]
Cell Types: Vero E6 Cell Tested Concentrations: 500 µM, 100 µM, 20 µM, 4 µM and 8 nM Incubation Duration: 26 hrs (hours) Experimental Results: Causes concentration-dependent reduction of virus (IC50=83 µM) 26 post-infection The nucleic acid concentration in the supernatant is 10-500 µM. Results in a concentration-dependent reduction of viral nucleic acid in the cytoplasm (IC50=119 µM) 26 hrs (hours) post-infection. Cell proliferation assay[6] Cell Types: Human HCC cell lines (HepG2 and SMMC-7721) and normal liver cells (L02 cells) Tested Concentrations: 0, 1, 2, 5, 10, 25, 50 and 100 µg/mL Incubation Duration: 24, 48 and 72 hrs (hours) Experimental Results: Inhibited cell proliferation in a time- and dose-dependent manner in HepG2 and SMMC-7721 cells. Cell cycle analysis[6] Cell Types: HepG2 and SMMC-7721 Cell Tested Concentrations: 0, 10, 25, 50 and 75 µg/mL Incubation Duration: 48 hrs (hours) Experimental Results: Significant increase in the number of HepG2 and SMMC-7721 cells in G0/G1 phase in a dose-dependent manner, and Dramatically diminished the numbe |
| Animal Protocol |
Fischer 344 rats (Four-month old, male, 290-330 g, 15 rats each group)
25 mg/kg Administration: IP, once daily for 3 days (the first dose at 15 min before surgery) Animal/Disease Models: Fischer 344 rats (4 months old, male, 290-330 g, 15 rats per group) [5] Doses: 25 mg/kg Route of Administration: IP, one time/day for 3 days (first dose in 15 minutes before administration) Experimental Results: Inhibited surgery-induced neuroinflammation and learning and memory impairment, increased GDNF (glial cell line-derived neuronal neuron) co-localized with hippocampal glial fibrillary acidic protein (an astrocyte marker) nutritional factors). Four-month old male Fischer 344 rats weighing 290 – 330 g were randomly assigned to: 1) control group (not being exposed to surgery or any drugs), 2) Amantadine group, 3) surgery group (right carotid artery exposure), and 4) surgery plus Amantadine group in the first experiment. Each group had 15 rats. In the second experiment, the rats were assigned to: 5) control group, 6) anti-GDNF antibody group, 7) surgery plus amantadine plus boiled anti-GDNF antibody group, and 8) surgery plus amantadine plus anti-GDNF antibody group. Each group had 8 rats. In the third experiment, the rats were randomly assigned to: 7) control group, 8) anesthesia only group, and 9) surgery plus GDNF group. Each group had 8 rats. GDNF and the anti-GDNF antibody were injected intracerebroventricularly. One week later, these rats were started to be tested in Barnes maze and then fear conditioning. Separate rats were assigned to 1) control group, 2) surgery group, and 3) surgery plus amantadine group (n = 6 per condition) and sacrificed at 6 h, 24 h or 10 days after the surgery for Western blotting and immunohistochemistry. Amantadine was dissolved in normal saline and injected intraperitoneally at 25 mg/kg/day for three days with the first dose at 15 min before surgery. Similar injections were performed in the amantadine only group except that no surgery and anesthesia were performed. The amantadine dose was chosen based on previous studies.[5] |
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion
Amantadine is well absorbed in the gastrointestinal tract after oral administration. It is primarily excreted unchanged in the urine via glomerular filtration and tubular secretion. 3–8 L/kg [healthy subjects] 0.2–0.3 L/hr/kg 0.10±0.04 L/hr/kg [healthy elderly men] It is rapidly and almost completely absorbed from the gastrointestinal tract. Amantadine can be distributed into breast milk. Excretion: Kidneys; >90% is excreted unchanged in the urine via glomerular filtration and tubular secretion. The excretion rate increases rapidly in acidic urine. Dialysis: Only a small amount (approximately 4%) is removed from the blood via hemodialysis. It is distributed in saliva, tear film, and nasal secretions; in animals, tissue concentrations (especially in the lungs) are higher than serum concentrations. It can cross the placenta and blood-brain barrier; it is distributed in breast milk. One patient's cerebrospinal fluid concentration was 52% of the corresponding plasma concentration. VolD - 4.4 ± 0.2 L/kg (normal renal function). 5.1 ± 0.2 L/kg (renal failure). For more complete data on the absorption, distribution, and excretion of amantadine (7 metabolites), please visit the HSDB record page. Metabolism/Metabolites No significant metabolism was found, but trace amounts of acetyl metabolites were identified. Eight amantadine metabolites were identified in human urine. One of these metabolites, the N-acetylated compound, was quantified in human urine at 5-15% of the administered dose. In 5 out of 12 healthy volunteers, the plasma concentration of acetylamantadine was 80% of the corresponding plasma amantadine concentration after administration of 200 mg amantadine. Acetylamantadine was not detected in the plasma of the remaining seven volunteers. Although trace amounts of acetyl metabolites were detected, no significant metabolism was found. Amantadine is well absorbed from the gastrointestinal tract after oral administration. Its anti-Parkinson's disease mechanism of action is not fully elucidated, but it appears to be achieved by promoting the release of dopamine from nerve endings in brain cells and stimulating a norepinephrine response. Its antiviral mechanism appears to be unrelated to this. The drug interferes with a viral protein, M2 (an ion channel), which is required for viral particles to "uncoat" after entering cells via endocytosis. Metabolites are excreted in the urine (A308). Elimination pathway: Primarily excreted unchanged via glomerular filtration and tubular secretion in the urine. Half-life: The mean half-life is 10 to 14 hours, but renal impairment significantly prolongs it to 7 to 10 days. The pharmacokinetics of amantadine were determined in 24 healthy adult male volunteers after oral administration of a single 100 mg amantadine hydrochloride soft capsule. The half-life is 17 ± 4 hours (range: 10 to 25 hours). In other studies, the mean plasma half-life of amantadine in 19 healthy volunteers was 16 ± 6 hours (range: 9 to 31 hours). Normal renal function: 11 to 15 hours. Elderly patients: 24 to 29 hours. Severe renal impairment: 7 to 10 days. Hemodialysis: 24 hours. When creatinine clearance is below 40 mL/min/1.73 m², the elimination half-life increases by 2 to 3 times or more; the mean half-life in patients undergoing long-term maintenance hemodialysis is 8 days. |
| Toxicity/Toxicokinetics |
Toxicity Summary
Its anti-Parkinson's disease mechanism of action is not fully elucidated, but it appears to work by promoting the release of dopamine from nerve endings in brain cells and stimulating a norepinephrine response. It also has NMDA receptor antagonistic activity. Its antiviral mechanism appears to be unrelated to this. The drug interferes with a viral protein, M2 (an ion channel), which is required for viral particles to "uncoat" after entering cells via endocytosis. Hepatotoxicity Despite its widespread use, there is little evidence that oral amantadine causes liver damage, whether from elevated serum enzymes or clinically apparent liver disease. Likelihood Score: E (Unlikely to cause clinically apparent liver damage). Pregnancy and Lactation Effects ◉ Overview of Use During Lactation Because amantadine may have negative effects on lactation, its use is best avoided during lactation. ◉ Effects on Breastfed Infants No relevant published information was found as of the revision date. ◉ Effects on lactation and breast milk Amantadine is a dopamine agonist. Clinical studies have shown that taking 100 mg of amantadine twice or three times daily can reduce serum prolactin levels and reduce galactorrhea in patients taking dopaminergic antipsychotics such as phenothiazines, haloperidol, and loxapine. [1][2] There are currently no reports on the effects of amantadine on milk production in lactating mothers. For mothers who have established lactation, their prolactin levels may not affect their ability to breastfeed. Protein binding Approximately 67% of the protein is bound to plasma proteins at concentrations ranging from 0.1 to 2.0 μg/mL. Toxicity Data LD50: 800 mg/kg (oral, rat) LD50: 700 mg/kg (oral, mouse) Interactions The anti-influenza A activity of amantadine and ribavirin, as well as the anti-influenza A activity of combined administration, were studied separately. In ferret tracheal ciliated epithelium, the combined use of the drugs synergistically delayed the virus-induced cytopathic effect.Concomitant use of alcohol and amantadine is not recommended, as this may increase the risk of central nervous system side effects such as dizziness, lightheadedness, orthostatic hypotension, or confusion.Concomitant use of anticholinergic drugs or other drugs with anticholinergic activity; tricyclic antidepressants; other anti-movement disorder drugs; antihistamines; or phenothiazines may enhance anticholinergic-like side effects, especially confusion, hallucinations, and nightmares; dosage adjustments of these drugs or amantadine may be necessary. In addition, patients should be advised to report any gastrointestinal problems promptly, as concurrent use of opioids may lead to paralytic ileus. Concomitant use of antidiarrheal medications containing both opioids and anticholinergics may enhance the anticholinergic-like side effects of amantadine; while significant interactions are unlikely with commonly used doses of antidiarrheal medications containing both opioids and anticholinergics, significant interactions may occur if these medications are abused. For more complete data on drug interactions of amantadine (one of 10), please visit the HSDB record page. |
| References | |
| Additional Infomation |
Amantadine hydrochloride may cause developmental toxicity depending on state or federal labeling requirements. Amantadine hydrochloride is the hydrochloride salt of amantadine, a synthetic tricyclic amine with antiviral, anti-Parkinson's disease, and anti-hyperalgesic activities. Amantadine appears to exert its anti-influenza A virus effect by interfering with the function of the transmembrane domain of the viral M2 protein, thereby preventing the release of infectious viral nucleic acid into host cells; additionally, the drug can also inhibit viral assembly during viral replication. Amantadine exerts its anti-Parkinson's disease effect by stimulating the release of dopamine from striatal dopaminergic nerve endings and inhibiting their presynaptic reuptake. The drug may exert some anticholinergic effects by inhibiting N-methyl-D-aspartate (NMDA) receptor-mediated acetylcholine stimulation, thereby producing an anti-hyperalgesic effect. It is an antiviral drug used for the prevention or treatment of influenza A. It is also used as an anti-Parkinson's disease drug to treat extrapyramidal reactions and postherpetic neuralgia. The mechanism by which it treats movement disorders is not fully understood, but it may reflect an increase in dopamine synthesis and release, and possibly an inhibition of dopamine uptake. See also: Amantadine (with the active moiety). Drug Indications Treatment of Parkinson's disease and Parkinsonian syndromes. Therapeutic Uses Anti-Parkinson's disease drug; antiviral drug; dopamine-like drug. Amantadine is used to treat certain fatigue symptoms associated with multiple sclerosis, including decreased energy, decreased well-being, poor concentration, memory loss, and decreased problem-solving abilities. /Not included in the US or Canadian product label/ Amantadine is indicated for the treatment of idiopathic Parkinson's syndrome (tremor paralysis; tremor paralysis), post-encephalitis Parkinson's syndrome, drug-induced extrapyramidal reactions, symptomatic Parkinson's syndrome following neurological damage caused by carbon monoxide poisoning, and Parkinson's syndrome associated with cerebral arteriosclerosis in the elderly. /US Product Label Includes/
Amantadine is indicated for the prevention and treatment of respiratory infections caused by influenza A virus strains. It is indicated for high-risk groups (including patients with lung or cardiovascular disease, the elderly, and residents of nursing homes and other long-term care facilities with chronic illnesses), close contacts of high-risk patients in hospital wards, immunocompromised patients, personnel in essential public service positions (e.g., police officers, firefighters, medical personnel), high-risk groups for whom influenza vaccination is contraindicated, and patients with severe influenza A virus infection. It is effective against all influenza A virus strains tested to date, including Russian, Brazilian, Texas, and London strains. It can be used concurrently with inactivated influenza A vaccines as a chemopreventive agent until protective antibodies are developed. However, it must be emphasized that annual vaccination of high-risk groups is the most important measure to reduce the impact of influenza. Currently, there are no rigorous controlled studies testing whether amantadine can prevent influenza A complications in high-risk groups. Drug-resistant influenza A virus strains have been reported in patients taking limantanide (amantadine); these resistant strains have apparently also been transmitted through household contact. Rimantadine and amantadine have similar chemical structures, antibacterial spectra, and mechanisms of action, and resistant viral strains exhibit cross-resistance to both amantadine and rimantadine. /US product label contains/ For more complete data on the therapeutic uses of amantadine (6 types), please visit the HSDB record page. Drug Warnings Swine influenza (H1N1) virus contains a unique combination of gene segments that have not been previously reported in swine or human influenza viruses in the United States or other regions. H1N1 virus is resistant to amantadine and ribavirin, but oseltamivir or zanamivir. Rare reports of suicide attempts (some fatal) have been reported in patients taking amantadine, many of whom were receiving short courses of the drug for influenza prevention or treatment. The manufacturer states that the incidence and pathophysiological mechanisms of these suicide attempts are unclear. Suicidal ideation or attempts have been reported in both patients with and without a history of mental illness. Amantadine may exacerbate the mental state of patients with a history of mental illness or substance abuse. Patients with suicidal tendencies may exhibit abnormal mental states, including disorientation, confusion, depression, personality changes, agitation, aggressive behavior, hallucinations, delusions, other psychotic reactions, somnolence, or insomnia. NMS (Neuro-Blocking Malignant Syndrome) has been reported in patients taking amantadine, and this condition is associated with dose reduction or discontinuation of the drug. NMS can be fatal and requires immediate intensive symptomatic and supportive care. Patients should be closely monitored when the amantadine dose is reduced or discontinued; this precaution is especially important for patients concurrently receiving antipsychotic medication. Nausea is one of the most common adverse reactions to amantadine; it has been reported in 5-10% of patients taking the drug at regular doses. Anorexia, constipation, diarrhea, and dry mouth are reported in 1-5% of patients taking amantadine, and vomiting is reported in up to 1%. Abdominal discomfort or dysphagia has also been reported. The incidence of gastrointestinal adverse reactions is comparable between amantadine and limantanide. For more complete data on drug warnings for amantadine (19 in total), please visit the HSDB records page. Pharmacodynamics Amantadine is an antiviral drug with anti-Parkinson's disease effects, often used in combination with levodopa when levodopa efficacy declines (possibly due to tolerance). Like the similar drug lymantadine, it is a derivative of adamantane. The mechanism of action of amantadine in treating Parkinson's disease and drug-induced extrapyramidal reactions is unclear. Studies have shown that amantadine can increase dopamine release in the brain of animals and does not have anticholinergic activity. Currently, there are three approved antiviral drugs for influenza in Japan: amantadine, zanamivir, and oseltamivir. These antiviral drugs can be used to control and prevent influenza, but they are not a substitute for vaccination. Amantadine is an antiviral drug effective against influenza A virus but ineffective against influenza B virus. Influenza A virus patients may shed susceptible virus in the early stages of treatment and resistant virus later, especially after 5-7 days of treatment. Even if resistant virus is present, these patients can still benefit from treatment. Amantadine susceptibility screening was performed using enzyme-linked immunosorbent assay, plaque reduction assay and TCID50/0.2 ml titration. The molecular changes associated with resistance have been identified as single nucleotide changes resulting in the substitution of one of the four key sites (amino acids 26, 27, 30 and 31) in the transmembrane region of the M2 protein. Polymerase chain reaction (PCR)-restriction fragment length polymorphism analysis was very effective. Resistant virus has emerged during outbreaks in nursing homes, and amantadine is used not only to treat influenza virus infection but also to treat Parkinson's disease. Measures should be taken to minimize contact between people taking antiviral drugs for treatment or chemoprevention and those not taking antiviral drugs. [1] Objective: To investigate how amantadine can be converted from an anti-influenza drug to an anti-Parkinson's disease drug. Methods: A review of historical literature on the use of amantadine from 1966 to the present. Results: Amantadine was initially introduced and used as an antiviral drug. A Parkinson's disease (PD) patient experienced symptom relief after taking amantadine to treat influenza. This discovery aroused interest and led to several important studies that eventually led to the discovery of new indications for amantadine. Conclusion: Amantadine has not been commonly used as a treatment for influenza for many years; however, it has become one of the commonly used drugs for the treatment of early Parkinson's disease symptoms and is also an option for the treatment of movement disorders. [2] Various animal models (most commonly mice), rabbits or monkeys have been used to screen compounds effective against orthopox virus infection. Treatment of vaccinia virus infection has been well studied in various models, including skin or eye scratch infection models, and intravenous, peritoneal, intracerebral or intranasal inoculation models. Vaccinia virus has been used in intranasal or aerosol infection studies to evaluate its therapeutic effect on fatal respiratory infections. The use of rabbitpox virus, monkeypox virus and smallpox virus in chemotherapy experiments is not as widespread as other viruses. A review of the literature over the past 50 years has revealed a variety of compounds that are effective in treating one or more of these infections, including thioaminoureas, nucleoside and nucleotide analogs, interferon, interferon inducers, and other unrelated compounds. The most promising anti-poxetine drugs are the acyclic nucleotides (S)-1-(3-hydroxy-2-phosphonomethoxypropyl)cytosine (Cidofovir, HPMPC) and 1-[((S)-2-hydroxy-2-oxo-1,4,2-dioxaphosphazenecycloheptane-5-yl)methyl]cytosine (cyclic HPMPC), and the acyclic nucleoside analog 2-amino-7-[(1,3-dihydroxy-2-propoxy)methyl]purine (S2242). Other classes of compounds that are under-studied in lethal infection models but warrant further attention include thioaminoureas associated with methionine, and analogs of adenosine-N(1)-oxide and 1-(benzyloxy)adenosine. [3] Background: Postoperative cognitive impairment is a clinical condition associated with poor prognosis. We investigated the efficacy of amantadine in alleviating surgery-induced cognitive impairment and the role of glial line-derived neurotrophic factor (GDNF) in this effect. Methods: Four-month-old male Fischer 344 rats underwent right carotid artery exposure surgery under intravenous anesthesia. Some rats were intraperitoneally injected with amantadine at 25 mg/kg/day for 3 consecutive days 15 minutes before surgery; or intraventricularly injected with GDNF or anti-GDNF antibody at the end of surgery. One week later, the rats were subjected to Barnes maze and fear conditioning tests. Hippocampal tissue was collected at 6 hours, 24 hours or 10 days after surgery for biochemical analysis. C8-B4 cells (a microglia) were pretreated with 1 ng/ml GDNF for 30 minutes and then treated with 5 ng/ml lipopolysaccharide for 2 hours. [5] In summary, amantadine inhibits viral replication in Vero E6 cell systems. In this study, due to the aforementioned limitations, we were unable to confirm that amantadine functionally interferes with the binding of the viral spike protein to ACE2 on target cells. This issue stems from the predicted tight binding of amantadine to Tyr489 and Phe456 in the SARS-CoV-2 receptor-binding domain (RBD); the interaction between the SARS-CoV-2 RBD (Arg319–Phe541 residues) and the N-terminal peptidase domain of ACE2 (Ser19–Asp615 residues) may suggest a potential antiviral mechanism of action for amantadine, but our data do not support this hypothesis from computer simulations. Inhibition of viral porins as another mechanism of action requires further investigation in future studies. In a recently published preprint, amantadine inhibited recombinant SARS-CoV-2 viral porin E and the putative SARS-CoV-2 viral porin Orf10. In an African Xenopus oocyte model, the authors observed that 10 µM amantadine inhibited the protein E ion channel-mediated current by up to 77%, which appears to be a stronger inhibitory effect on overall viral replication than the IC50 values (83–119 µM) observed in more complex eukaryotic cell culture models; these data suggest that viral porin inhibitors warrant further investigation. Finally, amantadine also appears to have an effect on known SARS-CoV-2 mutants to date, as protein E or Orf10 mutations were almost nonexistent or absent in SARS-CoV-2 mutant strains collected from Indian patients. Strain B 1.1.7 had neither protein E nor Orf10 mutations. However, even a single amino acid substitution can reduce the efficacy of small molecule drugs, as was the case with influenza A viruses many years ago. |
| Molecular Formula |
C10H18CLN
|
|
|---|---|---|
| Molecular Weight |
187.7
|
|
| Exact Mass |
187.112
|
|
| Elemental Analysis |
C, 63.99; H, 9.67; Cl, 18.89; N, 7.46
|
|
| CAS # |
665-66-7
|
|
| Related CAS # |
Amantadine; 768-94-5; Amantadine sulfate; 31377-23-8
|
|
| PubChem CID |
64150
|
|
| Appearance |
White to off-white solid powder
|
|
| Density |
1.067g/cm3
|
|
| Boiling Point |
225.7ºC at 760 mmHg
|
|
| Melting Point |
>300 °C(lit.)
|
|
| Flash Point |
96ºC
|
|
| Index of Refraction |
1.558
|
|
| LogP |
3.416
|
|
| Hydrogen Bond Donor Count |
2
|
|
| Hydrogen Bond Acceptor Count |
1
|
|
| Rotatable Bond Count |
0
|
|
| Heavy Atom Count |
12
|
|
| Complexity |
144
|
|
| Defined Atom Stereocenter Count |
0
|
|
| SMILES |
Cl[H].N([H])([H])C12C([H])([H])C3([H])C([H])([H])C([H])(C([H])([H])C([H])(C3([H])[H])C1([H])[H])C2([H])[H]
|
|
| InChi Key |
WOLHOYHSEKDWQH-UHFFFAOYSA-N
|
|
| InChi Code |
InChI=1S/C10H17N.ClH/c11-10-4-7-1-8(5-10)3-9(2-7)6-10;/h7-9H,1-6,11H2;1H
|
|
| Chemical Name |
adamantan-1-amine;hydrochloride
|
|
| Synonyms |
|
|
| HS Tariff Code |
2934.99.9001
|
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: Please store this product in a sealed and protected environment, avoid exposure to moisture. |
|
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
|
|||
|---|---|---|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: 6.88 mg/mL (36.65 mM) in PBS (add these co-solvents sequentially from left to right, and one by one), clear solution; with sonication (<60°C).
(Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 5.3277 mL | 26.6383 mL | 53.2765 mL | |
| 5 mM | 1.0655 mL | 5.3277 mL | 10.6553 mL | |
| 10 mM | 0.5328 mL | 2.6638 mL | 5.3277 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
A Safety and Efficacy Study of ADS-5102 in Patients With Multiple Sclerosis and Walking Impairment
CTID: NCT03567057
Phase: Phase 3 Status: Completed
Date: 2022-01-18
|
|
|
|
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved





























 COA
COA