| Size | Price | Stock | Qty |
|---|---|---|---|
| 10mg |
|
||
| 50mg | |||
| 100mg | |||
| Other Sizes |
































| Targets |
Protriptyline Hydrochloride primarily acts as a potent inhibitor of the re-uptake of norepinephrine and serotonin by nerve terminals. By blocking the transporters for these neurotransmitters, it increases their availability in the synaptic cleft. Unlike some other antidepressants, it does not block dopamine transport. However, it may have an indirect dopamine-facilitating effect through interactions of increased peri-synaptic abundance of norepinephrine, particularly in the cerebral cortex. This results in elevation of mood and behavioral activity.
|
|---|---|
| ln Vitro |
PC3 cells are cytotoxic to protriptyline hydrochloride (0-70 μM; 24 hours) [2].
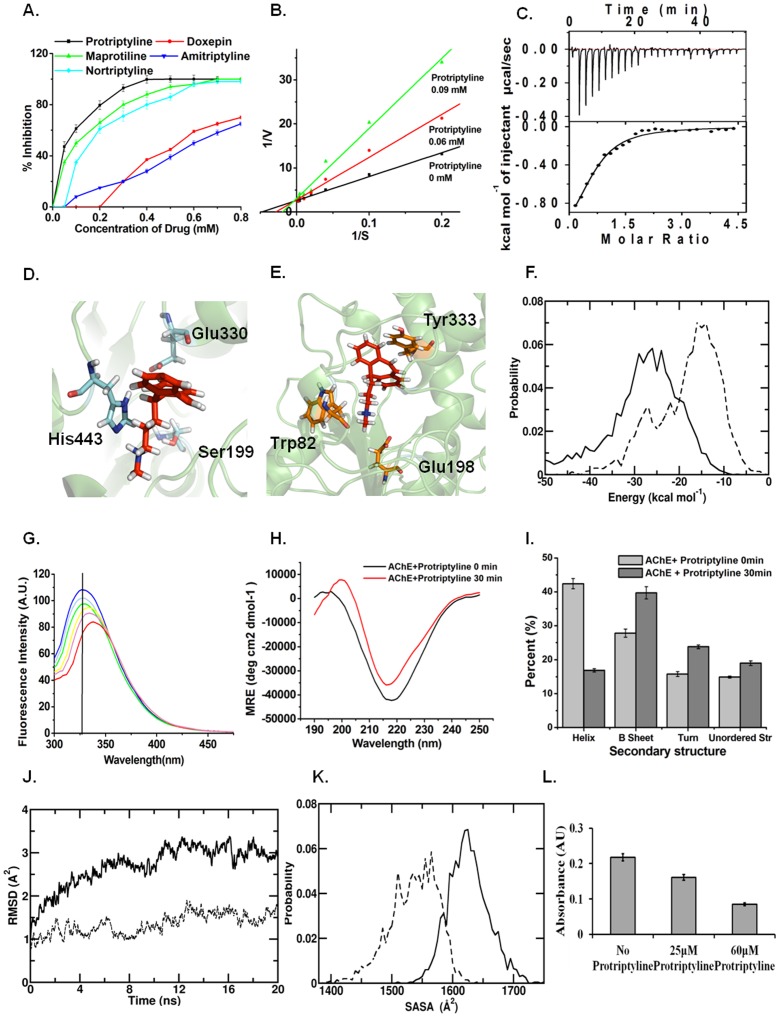
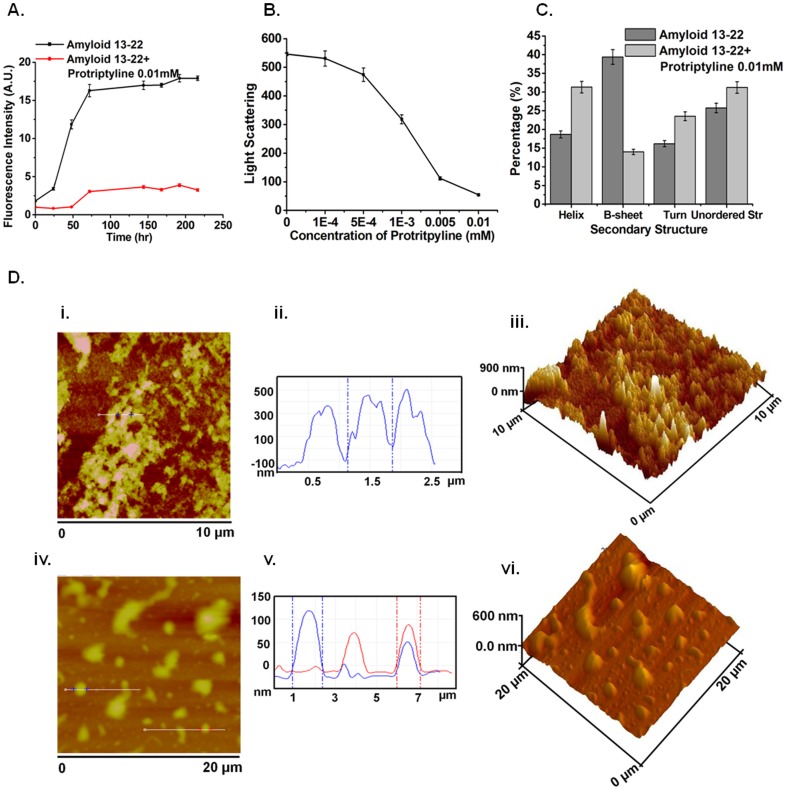
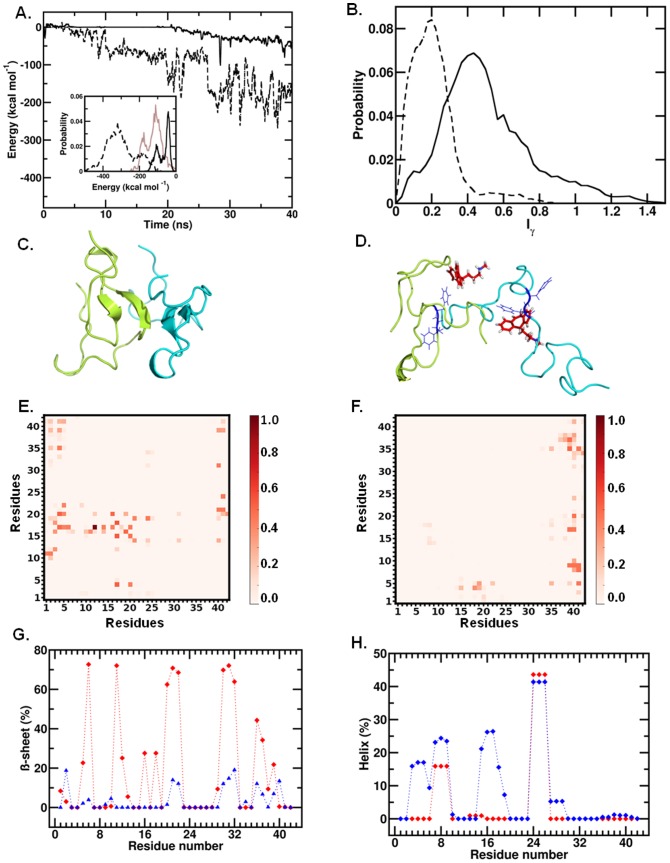
In vitro, Protriptyline Hydrochloride exhibits several activities. It inhibits acetylcholinesterase (AChE) with an IC50 value of 0.06 mM and inhibits Aβ self-assembly. It also possesses anticholinergic activity. Furthermore, as a TCA, it interacts with various receptors including histaminergic, cholinergic, and adrenergic receptors, contributing to its side effect profile. Its primary in vitro effect is on neurotransmitter reuptake, which is studied using synaptosomal preparations or cell lines expressing the norepinephrine and serotonin transporters. |
| ln Vivo |
Protriptyline hydrochloride (10 mg/kg; intraperitoneal injection; 21 days; AD rat model) improves spatial learning and retained memory in STZ-treated rats [3].
In vivo, Protriptyline Hydrochloride is used clinically as an antidepressant. Its therapeutic effects are attributed to the enhanced noradrenergic and serotonergic neurotransmission in the brain. It has also been investigated for the treatment of obstructive sleep apnea/hypopnea syndrome (OSAHS). Its in vivo effects include elevation of mood and increased behavioral activity. The drug's "activating" property is a key characteristic that distinguishes it from more sedating TCAs, making it useful for patients with psychomotor retardation. |
| Enzyme Assay |
Cell-free assays for Protriptyline Hydrochloride focus on its primary mechanism of action, which is the inhibition of neurotransmitter transporters. To measure this, a common assay involves preparing membrane fractions from brain tissue or from cells that express the human norepinephrine transporter (NET) or serotonin transporter (SERT). These membranes are incubated with radiolabeled neurotransmitters (e.g., [3H]-norepinephrine or [3H]-serotonin) in the presence of varying concentrations of Protriptyline. The amount of radiolabeled neurotransmitter taken up into the membranes is measured, and the inhibition constant (IC50) is calculated. This assay directly quantifies the compound's potency as a reuptake inhibitor.
|
| Cell Assay |
Cytotoxicity assay[2]
Cell Types: PC3 Cell Tested Concentrations: 50, 60 and 70 μM Incubation Duration: 24 hrs (hours) Experimental Results: Cell viability diminished in a concentration-dependent manner. In vitro cell-based assays for Protriptyline Hydrochloride are designed to study its effects on neuronal cells. Cell lines like SH-SY5Y (neuroblastoma) or primary neuronal cultures are treated with the compound. The effect on neurotransmitter uptake can be measured by adding fluorescent or radiolabeled neurotransmitters to the media and quantifying the amount internalized by the cells. Furthermore, the compound's effect on cell signaling pathways, such as the cAMP pathway, can be assessed. Its cytotoxicity and effects on cell viability can also be evaluated using standard assays like MTT, particularly when studying its potential neuroprotective or neurotoxic effects. |
| Animal Protocol |
Animal/Disease Models: AD rat model [3]
Doses: 10 mg/kg Route of Administration: intraperitoneal (ip) injection; 21 days. Experimental Results: diminished pTau, Aβ42 and BACE-1 levels, neurodegeneration, oxidative stress and glial activation. By reducing NFκB and GFAP expression, improving p-ERK/ERK ratio and increasing BDNF and CREB levels. The in vivo activity of Protriptyline Hydrochloride is primarily validated through its clinical use and animal models of depression. In preclinical research, the forced swim test and tail suspension test in rodents are classic models used to evaluate antidepressant-like activity. Protriptyline would be administered to animals, and the reduction in immobility time is measured as an indicator of antidepressant efficacy. For its off-label use in conditions like OSAHS, animal models of sleep apnea are used to study its effect on respiratory function. The drug's pharmacokinetic and pharmacodynamic properties are well-characterized in humans. |
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion
Protriptyline has been reported to be excreted cumulatively in the urine over 16 days, accounting for approximately 50% of the total dose. Fecal excretion appears to play a minimal role in drug clearance. Excretion is rapid, a stark contrast to the drug's slow onset of action. /Tricyclic antidepressants/ …easily absorbed from the gastrointestinal tract. …rapidly distributed and metabolized via demethylation, oxidation, and aromatic hydroxylation. In the urine of rats treated with protriptyline, the excretion of 10,11-dihydro-10,11-epoxy-5-(3-methylaminopropyl)-5H-dibenzo[A,D]cycloheptene was twice that of 10,11-dihydro-10,11-epoxy-5-(3-aminopropyl)-5H-dibenzo[A,D]cycloheptene, and the two together accounted for 40% of the protriptyline dose. Patients taking nitrazepam concurrently did not show a significant difference in mean plasma concentrations of protriptyline compared to those not taking nitrazepam. Patients receiving sodium pentobarbital showed a significantly lower mean plasma concentration. Early values may be predictive, allowing for early dose adjustments. Metabolisms/Metabolites It is known that the 10,11 double bond of protriptyline undergoes oxidation in humans, miniature pigs, and dogs… Two metabolites have been detected, indicating the presence of an epoxide intermediate, namely dihydrodiol, and a rearrangement product formed via… a cationic intermediate… rearranged to a dihydroanthracene structure. Three urinary metabolites have been identified in dogs, miniature pigs, and humans: 10-hydroxy-N-methyl-5H-dibenzo[A,D]cycloheptene-5-propanediamine, 10,11-dihydroxy-N-methyl-5H-dibenzo[A,D]cycloheptene-5-propanediamine, and 5,10-dihydroxy-10-formylanthracene-5-propanediamine. ...Protriptyline...can lead to the presence of 10,11-oxides in urine. In the urine of rats treated with protriptyline...two metabolites have been identified...10,11-dihydroxy-10,11-epoxy-5-(3-methylethylaminopropyl)-5H-dibenzo[A,D]cycloheptene and 10,11-dihydro-10,11-epoxy-5-(3-aminopropyl)-5H-dibenzo[A,D]cycloheptene. Elimination pathway: Approximately 50% of the total drug is excreted in the urine over 16 days. Fecal excretion does not appear to be significant. Biological half-life In 8 subjects, after a single oral dose of 30 mg, the peak plasma concentrations ranged from 10.4 to 22.3 ng/ml 6–12 hours post-administration. The mean half-life (T/2) was 74.3 hours, with individual subjects experiencing a range of 53.6–91.7 hours. Eight subjects underwent a single oral administration of protriptyline hydrochloride. Assuming complete absorption, the estimated first-pass metabolism was relatively small, ranging from 10–25% of the dose. The mean volume of distribution was 22.5 L/kg, ranging from 15.0–31.2 L/kg. The conclusion is that a longer half-life is associated with a smaller first-pass metabolism. Plasma drug concentrations in 30 subjects: After 3.5 weeks of treatment with 40 mg daily, plasma concentrations ranged from 430–1430 nanomoles/L. A single-dose study in five volunteers showed little inter-individual variation in the volume of distribution of protriptyline. However, the half-life (T2) may vary, ranging from 54–198 hours. Protriptyline Hydrochloride is well-absorbed after oral administration. It undergoes extensive first-pass metabolism in the liver. It is highly protein-bound (around 90%) and has a large volume of distribution. The drug is metabolized primarily by hepatic cytochrome P450 enzymes, including CYP2D6, to active and inactive metabolites. Its half-life is relatively long, ranging from 50 to 100 hours, allowing for once-daily dosing. It is excreted in the urine and feces. Due to its long half-life and active metabolites, its pharmacokinetics are complex and subject to genetic polymorphisms in metabolic enzymes. |
| Toxicity/Toxicokinetics |
Hepatotoxicity
It has been reported that 10% to 12% of patients taking tricyclic antidepressants experience abnormal liver function, but elevations of liver enzymes exceeding three times the upper limit of normal are uncommon. Transaminase abnormalities are usually mild, asymptomatic, and transient, and return to normal with continued medication. The incidence of serum enzyme elevations during protriptyline treatment is unclear. There have been reports of clinically significant acute liver injury in patients taking tricyclic antidepressants, but there are currently no specific reports related to protriptyline. The typical latency period for acute liver injury caused by tricyclic antidepressants is 1 to 14 months. The pattern of serum enzyme elevation is usually cholestatic, but hepatocellular cases have also been reported, including acute hepatitis-like syndrome with acute liver failure. Cases of acute cholestatic hepatitis and persistent jaundice consistent with disappearance of bile duct syndrome have been associated with other tricyclic antidepressants, primarily amitriptyline and imipramine, the two most commonly used drugs in this class. In reported cases, signs or symptoms of allergic reactions (rash, fever, and eosinophilia) are common, but these symptoms are usually mild and transient. Autoantibody formation is rare. Protriptyline is a rarely used tricyclic antidepressant, but its adverse reaction spectrum is suspected to be similar to that of imipramine and amitriptyline. Probability score: E (Unproven, but suspected as a rare cause of clinically significant liver damage). Effects during pregnancy and lactation: ◉ Overview of use during lactation: Since there is no published experience with the use of protriptyline during lactation, other medications may be preferred, especially when breastfeeding newborns or premature infants. ◉ Effects on breastfed infants: As of the revision date, no published information on protriptyline was found. A study of 20 breastfed infants born to mothers taking tricyclic antidepressants, followed for 1 to 3 years, found no adverse effects on infant growth and development. Two small controlled studies have shown that other tricyclic antidepressants have no adverse effects on infant development. Another study formally tested 25 infants whose mothers took tricyclic antidepressants during pregnancy and lactation for 15 to 71 months, finding that these infants grew and developed normally. ◉ Effects on Lactation and Breast Milk An observational study investigated the outcomes of 2,859 women who took antidepressants in the two years prior to pregnancy. Compared to women who did not take antidepressants during pregnancy, mothers who took antidepressants in all three stages of pregnancy were 37% less likely to breastfeed at discharge. Mothers who took antidepressants only in the third trimester were 75% less likely to breastfeed at discharge. Mothers who took antidepressants only in the first and second trimesters were not less likely to breastfeed at discharge. The specific antidepressants used by the mothers were not specified. A retrospective cohort study analyzed hospital electronic medical records from 2001 to 2008, comparing women who took antidepressants in late pregnancy (n = 575), women with mental illness but not taking antidepressants (n = 1552), and mothers not diagnosed with mental illness (n = 30,535). Results showed that women who took antidepressants were 37% less likely to breastfeed at discharge than women not diagnosed with mental illness, but there was no significant difference in the likelihood of breastfeeding compared to untreated mothers with mental illness. None of the mothers were taking protriptyline. A study of 80,882 Norwegian mother-infant pairs from 1999 to 2008 showed that 392 women reported starting antidepressants postpartum, and another 201 women reported starting antidepressants during pregnancy. Compared to a control group not exposed to antidepressants, taking antidepressants in late pregnancy was associated with a 7% lower rate of breastfeeding initiation, but had no effect on the duration of breastfeeding or the rate of exclusive breastfeeding. Compared to the control group who were not exposed to antidepressants, starting or restarting antidepressant medication postpartum was associated with a 63% lower rate of primary breastfeeding at 6 months, a 51% lower rate of any feeding method, and a 2.6-fold increased risk of abruptly stopping breastfeeding. The study did not specify the type of antidepressant. The toxicity of Protriptyline Hydrochloride is consistent with other tricyclic antidepressants. Overdose can be life-threatening, leading to cardiac arrhythmias, seizures, and severe anticholinergic effects. Common side effects at therapeutic doses include dry mouth, blurred vision, constipation, urinary retention, sedation (though less than with other TCAs), and orthostatic hypotension. It carries a boxed warning for an increased risk of suicidal thinking and behavior in children, adolescents, and young adults. Chronic use can lead to weight gain and sexual dysfunction. It is contraindicated in patients with recent myocardial infarction. |
| References |
|
| Additional Infomation |
Protriptyline is a carbon-tricyclic compound with antidepressant effects. It is derived from the hydride of dibenzo[a,d][7]annulene. Protriptyline hydrochloride is a dibenzocyclohepten derivative tricyclic antidepressant (TCA). TCAs have a structure similar to phenothiazine drugs, containing a tricyclic ring system with an alkylamine substituent attached to the central ring. In non-depressed patients, protriptyline does not affect mood or arousal but may cause sedation. In depressive patients, protriptyline has a positive effect on mood. TCAs are potent inhibitors of serotonin and norepinephrine reuptake. Furthermore, long-term use of TCAs downregulates cortical β-adrenergic receptors and sensitizes postsynaptic serotonergic receptors. The antidepressant effect of tricyclic antidepressants (TCAs) is thought to be due to an overall enhancement of serotonergic neurotransmission. TCAs can also block histamine H1 receptors, α1-adrenergic receptors, and muscarinic receptors, resulting in their sedative, hypotensive, and anticholinergic effects (e.g., blurred vision, dry mouth, constipation, urinary retention), respectively. For a complete list of side effects, please see the Toxicity section below. Protriptyline is used to treat depression. Protriptyline is a tricyclic antidepressant. Protriptyline is a tricyclic antidepressant that has been widely used to treat major depressive disorder. Most tricyclic antidepressants have been shown to cause a low incidence of mild, transient elevations in serum enzymes, and rare, clinically significant acute cholestatic liver injury. However, the potential hepatotoxicity of protriptyline has not been fully elucidated. Protriptyline hydrochloride is a dibenzocyclohepten derivative tricyclic antidepressant (TCA). TCAs have a structure similar to phenothiazines, both containing a tricyclic ring system with an alkylamine substituent attached to the central ring. In non-depressive patients, protriptyline does not affect mood or arousal but may cause sedation. Protriptyline has a positive effect on mood in patients with depression. TCAs are potent inhibitors of serotonin and norepinephrine reuptake. Furthermore, long-term use of TCAs downregulates cortical β-adrenergic receptors and sensitizes postsynaptic serotonergic receptors. The antidepressant effect of TCAs is thought to be due to an overall enhancement of serotonergic neurotransmission. Tricyclic antidepressants (TCAs) also block histamine H1 receptors, α1-adrenergic receptors, and muscarinic receptors, resulting in their sedative, hypotensive, and anticholinergic effects (e.g., blurred vision, dry mouth, constipation, urinary retention), respectively. For a complete list of side effects, see the Toxicity section below. Protriptyline can be used to treat depression.
Tricyclic antidepressants, with effects and side effects similar to imipramine.It may cause excitement. See also: Protriptyline hydrochloride (salt form). Drug Indications For the treatment of depression. Mechanism of Action Protriptyline works by reducing the reuptake of norepinephrine and serotonin (5-HT). The effects of tricyclic antidepressants on the metabolism of catecholamines and indoleamines in the brain have made significant contributions to the "bioamine hypothesis" of depression. ...All drugs block the reuptake of norepinephrine at adrenergic nerve endings. Demethylated analogues are more potent in this effect. Tricyclic antidepressants Protriptyline Hydrochloride is an FDA-approved drug, indicated primarily for the treatment of depression. Its "activating" profile makes it a first-line choice for patients with depression characterized by lethargy and withdrawal. It is also used off-label for ADHD, narcolepsy, and OSAHS. The drug is available in tablet form under various brand names, including Vivactil. As a tricyclic antidepressant, it has largely been superseded by newer agents like SSRIs and SNRIs due to its more severe side effect profile and toxicity in overdose. However, it remains a valuable option for treatment-resistant cases. All information is for research reference and not for diagnostic or clinical use. |
| Molecular Formula |
C19H22CLN
|
|---|---|
| Molecular Weight |
299.84
|
| Exact Mass |
299.144
|
| CAS # |
1225-55-4
|
| Related CAS # |
Protriptyline;438-60-8;Protriptyline (N-methyl-d3) (hydrochloride);1435934-21-6
|
| PubChem CID |
4976
|
| Appearance |
White to off-white solid powder
|
| Boiling Point |
407.7ºC at 760 mmHg
|
| Melting Point |
169-171°
|
| Flash Point |
198.3ºC
|
| Vapour Pressure |
7.41E-07mmHg at 25°C
|
| LogP |
5.494
|
| Hydrogen Bond Donor Count |
1
|
| Hydrogen Bond Acceptor Count |
1
|
| Rotatable Bond Count |
4
|
| Heavy Atom Count |
20
|
| Complexity |
296
|
| Defined Atom Stereocenter Count |
0
|
| InChi Key |
BWPIARFWQZKAIA-UHFFFAOYSA-N
|
| InChi Code |
InChI=1S/C19H21N/c1-20-14-6-11-19-17-9-4-2-7-15(17)12-13-16-8-3-5-10-18(16)19/h2-5,7-10,12-13,19-20H,6,11,14H2,1H3
|
| Chemical Name |
N-methyl-3-(2-tricyclo[9.4.0.03,8]pentadeca-1(15),3,5,7,9,11,13-heptaenyl)propan-1-amine
|
| HS Tariff Code |
2934.99.9001
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: Please store this product in a sealed and protected environment, avoid exposure to moisture. |
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
DMSO : ~250 mg/mL (~833.78 mM)
H2O : ~100 mg/mL (~333.51 mM) |
|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.08 mg/mL (6.94 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution.
For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 20.8 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.08 mg/mL (6.94 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 20.8 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. View More
Solubility in Formulation 3: ≥ 2.08 mg/mL (6.94 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. Solubility in Formulation 4: 100 mg/mL (333.51 mM) in PBS (add these co-solvents sequentially from left to right, and one by one), clear solution; with ultrasonication. |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 3.3351 mL | 16.6756 mL | 33.3511 mL | |
| 5 mM | 0.6670 mL | 3.3351 mL | 6.6702 mL | |
| 10 mM | 0.3335 mL | 1.6676 mL | 3.3351 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
|
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved