| Size | Price | Stock | Qty |
|---|---|---|---|
| 1mg |
|
||
| 5mg |
|
||
| 10mg |
|
||
| 25mg | |||
| Other Sizes |
































Purity: ≥98%
Pasireotide acetate (formerly SOM230), the acetate salt of Pasireotide, is a stable cyclohexapeptide somatostatin derivative that exhibits unique high-affinity binding to human somatostatin receptors (subtypes sst1/2/3/4/5, pKi=8.2/9.0/9.1/<7.0/9.9 respectively). It is an orphan drug approved for the treatment of Cushing's disease in patients who fail or are ineligible for surgical therapy. It was developed by Novartis. Pasireotide is a somatostatin analogue with a 40-fold increased affinity to somatostatin receptor 5 compared to other somatostatin analogues.
| Targets |
sst1 ( pKi = 8.2 ); sst2 ( pKi = 9.0 ); sst3 ( pKi = 9.1 ); sst4 ( pKi < 7.0 ); sst5 ( pKi = 9.9 )
|
|---|---|
| ln Vitro |
Pasireotide acetate binds to the human somatostatin receptor (subtype sst1/2/3/4/5, pKi=8.2/9.0/9.1/<7.0/9.9) with a particularly high affinity [1]. GH release in primary cultures of pituitary cells stimulated by growth hormone (GRH) with an IC50 of 0.4 nM [1].
The strategy pursued in this research has been rewarded with the demonstrated superiority of Pasireotide/25 compared to 2. Pharmacological studies in vitro have clearly shown that Pasireotide/25 effectively inhibited the growth hormone releasing hormone (GHRH) induced growth hormone (GH) release in primary cultures of rat pituitary cells with an IC50 of 0.4 ± 0.1 nmol/L (n = 5) [1]. Pasireotide is a somatostatin analogue with high binding affinity to somatostatin receptor subtypes sst1,2,3 and sst5, as shown in competitive binding studies using CHO-K1 cells expressing human recombinant somatostatin receptors (Table 2) (Bruns et al., 2002, Schmid and Schoeffter, 2004). In CCL39 cells expressing human recombinant sst receptors, pasireotide and somatostatin (SRIF-14) inhibited forskolin-stimulated cAMP accumulation with approximately the same efficacy and potency. Compared with octreotide, the functional activity (based on EC50 values) of pasireotide on sst1, sst3 and sst5 was >30-, 11- and 158-fold higher, respectively, but 7-fold lower on sst2 (Schmid and Schoeffter, 2004). Based on the differences in binding affinity and functional activity of Pasireotide and octreotide, it can be speculated that in cells and tissues that express sst receptors other than the sst2 receptor subtype, pasireotide will have a stronger inhibitory effect on hormone secretion than octreotide [3]. |
| ln Vivo |
Pasireotide acetate (160 mg/kg/month; subcutaneously for 4 months) dramatically decreases plasma insulin, boosts plasma plasma levels, reduces tumor growth, and increases Pdx1-Cre cells [2]. Pasireotide acetate (2-50 μg/kg; subcutaneously, twice daily for 42 days) produces analgesic and anti-inflammatory effects via SSTR2 receptors in immune-mediated arthritis models [4].
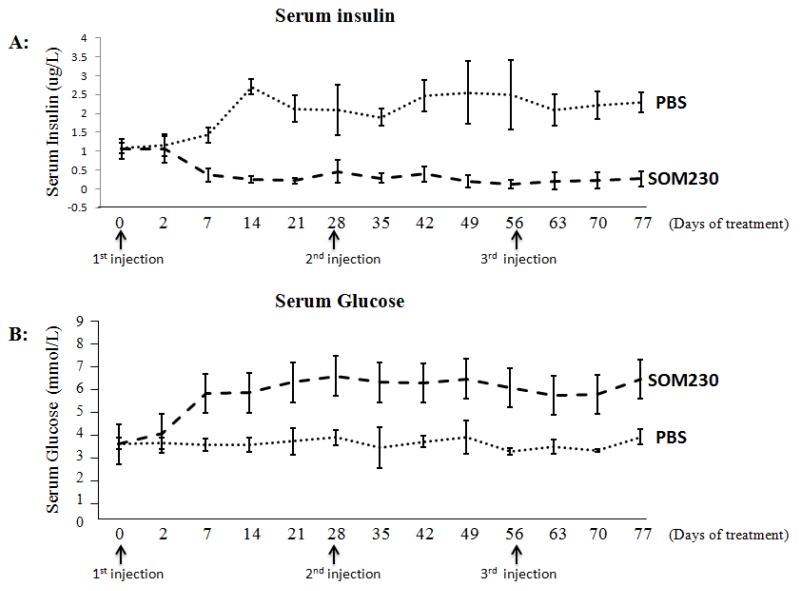
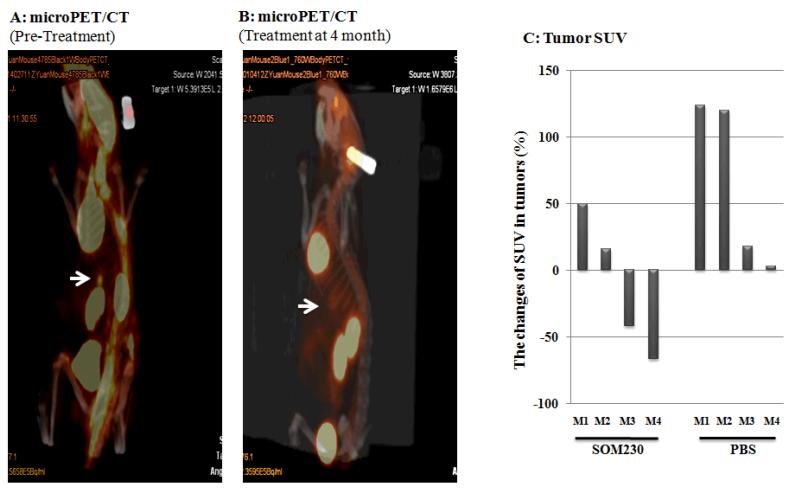
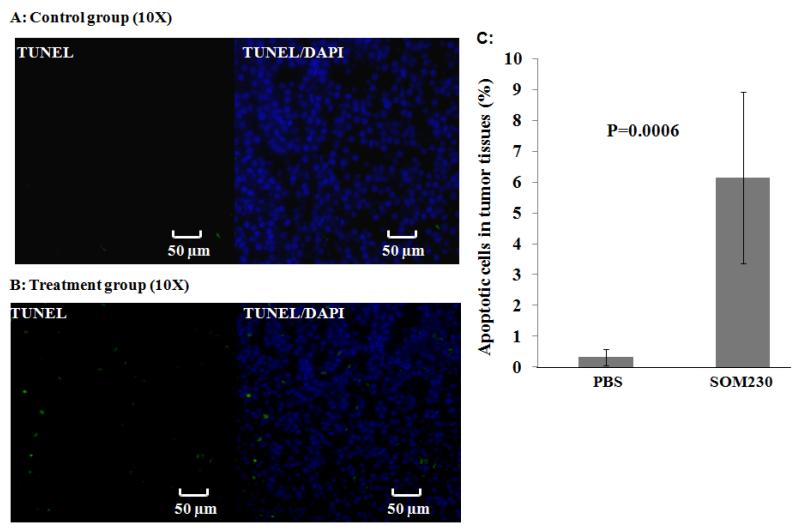
In vivo, Pasireotide/25 also potently suppressed GH secretion in rats. The ED50 values determined at 1 and 6 h after injection of 25 indicated its very long duration of action in vivo. In the rat, 25 strongly decreases IGF-1 plasma levels, with the efficacy being markedly enhanced compared with the effects elicited by 2 after 7 days of treatment. Furthermore, in rats, dogs, and rhesus monkeys, 25 potently and dose-dependently decreased IGF-1 levels for prolonged periods of time without desensitization as observed with SMS 201-995 (2).[1] Background: Pasireotide (SOM230), a long-acting somatostatin analogue (LAR), has improved agonist activity at somatostatin receptors. We tested the effect of SOM230 on insulin secretion, serum glucose concentrations, tumor growth, and survival using an MEN1 transgenic mouse model. Methods: Eight 12-month-old conditional Men1 knockout mice with insulinoma were assessed. The treatment (n = 4) and control groups (n = 4) received monthly subcutaneous injections of SOM230 or PBS. Serum insulin and glucose levels were determined by enzyme-linked immunosorbent assay and enzymatic colorimetric assay, respectively. Tumor activity, growth, and apoptosis were determined by microPET/CT scan and histologic analysis. Results: On day 7, there was a decrease in serum insulin levels from 1.06 ± 0.28 μg/L to 0.37 ± 0.17 μg/L (P = .0128) and a significant increase in serum glucose from 4.2 ± 0.45 mmol/L to 7.12 ± 1.06 mmol/L (P = .0075) in the treatment group but no change in the control group. Tumor size was less in the treatment group (2,098 ± 388 μm(2)) compared with the control group (7,067 ± 955 μm(2); P = .0024). Furthermore, apoptosis was increased in the treatment group (6.9 ± 1.23%) compared with the control group (0.29 ± 0.103%; P = .002). Conclusion: SOM230 demonstrates antisecretory, antiproliferative, and proapoptotic activity in our MEN1 model of insulinoma. Further studies of the effects of SOM230 in PNET patients with MEN1 mutations are warranted.[2] Objective: Clinical and preclinical evidence suggests that somatostatin exhibits potent antiinflammatory and antinociceptive properties. However, it is not known which of the 5 somatostatin receptor subtypes (SSTRs 1-5) is involved in these actions. The purpose of this study was to assess the effects of the stable somatostatin analogs octreotide and Pasireotide (SOM230) in a mouse model of antigen-induced arthritis (AIA). Methods: Studies were performed in SSTR2-deficient mice (SSTR2(-/-)) and their wild-type littermates (SSTR2(+/+)). The expression of SSTR1, SSTR2A, SSTR3, and SSTR5 in dorsal root ganglia was examined by immunohistochemistry. Results: Untreated SSTR2(-/-) mice with AIA displayed joint swelling and mechanical hyperalgesia similar to that seen in SSTR2(+/+) mice. In wild-type mice, both octreotide and Pasireotide significantly attenuated knee joint swelling and histopathologic manifestations of arthritis to an extent comparable to that of dexamethasone. In SSTR2(-/-) mice, the antiinflammatory effects of both octreotide and pasireotide were completely abrogated. Prolonged administration of Pasireotide also inhibited joint swelling and protected against joint destruction during AIA flare reactions. In addition, both octreotide and pasireotide reduced inflammatory hyperalgesia. The antinociceptive actions of octreotide were abolished in SSTR2(-/-) mice, but those of pasireotide were retained. In dorsal root ganglia of naive wild-type mice, only SSTR1 and SSTR2A, but not SSTR3 or SSTR5, were detected in a subset of small- and medium-diameter neurons. Conclusion: Our findings indicate that the antinociceptive and antiinflammatory actions of octreotide and Pasireotide are largely mediated via the SSTR2 receptor. In addition, we identified the SSTR1 receptor as a novel pharmacologic target for somatostatin-mediated peripheral analgesia in inflammatory pain [4]. |
| Enzyme Assay |
Pharmacological Characterization. Radioligand Binding Assays. [1]
Radioligand binding assays were performed as described previously. Briefly, membranes from CHO and COS cells expressing the respective human SRIF receptor subtype were incubated with the SRIF receptor ligand Tyr11[125I]-SRIF in the presence or absence of various concentrations of SRIF receptor ligands. The incubation was stopped after 1 h by rapid filtration through Whatman GF/C filters. Inhibition curves were analyzed, and IC50 values were calculated. |
| Cell Assay |
Apoptosis analysis [2]
Apoptotic status in endocrine tumor tissues was measured in control and treated mice by Terminal deoxynucleotidyl transferase dUTP Nick End-Labeling (TUNEL) assay. For quantification of apoptosis, the TUNEL assay was performed according to the manufacturer on paraffin-embedded sections with an In Situ Cell Death Detection Kit. The tissue sections were deparaffinized and treated with proteinase K (10 μg/ml) for 20 min. The sections were then washed twice with PBS, labeled and stained with the TUNEL reaction mixture (label plus enzyme solutions) for 60 min at 37°C, and washed twice with PBS in the dark. The slides were mounted in Vectashield mounting medium with DAPI. The apoptotic fluorescent cells were counted under a fluorescent microscope and the numbers were expressed as the percentage of total cells ± standard deviation (SD). A negative control without enzyme treatment and a positive control with DNase I treatment were also performed. SSTR detection [2] The detection of sstr1-5 in pancreatic endocrine tumor tissue was measured in our mouse model. Immunofluorescent (IF) staining for sstr1-5 on sections was performed using rabbit or goat anti-sstr1, sstr2, sstr3, sstr4, and sstr5 antibodies (Abs) and were incubated at a 1:50 dilution overnight at 4° C, respectively. Pig anti-insulin Ab was also used for identification of β-cells. Sections were then washed with PBS and were incubated with a 1:200 dilution of anti-rabbit or anti-goat Alexa Fluor 488 and anti-pig Alexa Fluor 647 secondary antibodies for 45 min in the dark, respectively. A negative control without primary antibody was also performed. |
| Animal Protocol |
Animal/Disease Models: 12-month-old conditional Men1 gene knockout mice with insulinoma [2]
Doses: 160 mg/kg/oral Route of Administration: monthly subcutaneous injection for 4 months Experimental Results: diminished serum insulin from 1.060 μg/L to 0.3653 μg/L, increasing serum glucose from 4.246 mM to 7.122 mM. Dramatically diminished tumor size and increased apoptosis. SOM230/Pasireotide and PBS Administration [2] Mice were anesthetized using halothane and then shaved on their flank for subcutaneous injection of either phosphate buffered saline (PBS) buffer or Pasireotide/SOM230 at a concentration of 160mg/Kg/month (64mg/ml) every month for 4 months. Treatment protocol and drugs. [4] Mice were randomly allocated to the following groups (8–10 animals per experimental condition): 0.9% saline; 2, 20, or 50 μg/kg of octreotide; or 2, 20, or 50 μg/kg of Pasireotide. These doses have been shown to elicit long-lasting therapeutic effects on pituitary hormone secretion in rodents and humans. Octreotide and Pasireotide were a kind gift from Novartis and were administered subcutaneously in a volume of 0.1 ml/kg of body weight. Treatment was started 12 hours before the induction of AIA and was continued for 3, 21, or 42 days, with administration every 12 hours for the indicated time periods. Flare reactions were provoked by injecting the right knee joint cavity with 100 μg of mBSA dissolved in 20 μl of PBS on days 21 and 35 of AIA. An additional group received 0.6 mg/kg of dexamethasone palmitate by intraperitoneal injection. Dexamethasone treatment was carried out for 5 days, followed by a 2-day pause starting 12 hours before AIA induction. |
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion
Peak plasma concentrations of parecide are reached within 0.25–0.5 hours. Cmax and AUC increase proportionally to the dose after single and multiple administrations. Parecide is primarily cleared by the liver (biliary excretion) (approximately 48%), with a small amount cleared by the kidneys (approximately 7.63%). Parecide has a wide distribution, with a volume of distribution >100 L. The clearance rate in healthy subjects is approximately 7.6 L/h, and in patients with Cushing's disease, it is approximately 3.8 L/h. Metabolisms/Metabolites Metabolism is minimal. Biological Half-Life The half-life is 12 hours. |
| Toxicity/Toxicokinetics |
Effects During Pregnancy and Lactation
◉ Overview of Use During Lactation The secretion of paretin into breast milk has not been studied. However, due to its high molecular weight of 1047 Daltons, very little is likely secreted into breast milk, and as a peptide drug, it is likely to be digested in the infant's gastrointestinal tract. It is unlikely to reach clinically significant concentrations in infant serum. However, the manufacturer states that paretin should not be used by breastfeeding women. Alternative medications are recommended. ◉ Effects on Breastfed Infants No relevant published information was found as of the revision date. ◉ Effects on Lactation and Breast Milk No relevant published information was found as of the revision date. |
| References |
|
| Additional Infomation |
Pasireotide is a hexacyclic hexapeptide composed of L-phenylglycyl, D-tryptophanyl, L-lysyl, O-benzyl-L-tyrosyl, L-phenylalanyl, and modified L-hydroxyproline residues linked in sequence. It is a somatostatin analog with pharmacological properties similar to the natural hormone somatostatin; it is used to treat Cushing's disease (in its diaspartate form). It also has antitumor activity. It is a homocyclic peptide and also a peptide hormone. It is the conjugate base of Pasireotide (2+). Pasireotide is a synthetic, long-acting cyclic hexapeptide with somatostatin-like activity. It is marketed as the diaspartate form of Signifor for the treatment of Cushing's disease. Pasireotide is a somatostatin analog. The mechanism of action of Pasireotide is as a somatostatin receptor agonist. Pasireotide is a synthetic somatostatin polypeptide analog with an ability to inhibit the levels and activity of growth hormone, insulin, glucagon, and many other gastrointestinal peptides similar to that of the natural hormone. Because of its longer half-life than somatostatin, parretin can be used clinically to treat pituitary neuroendocrine tumors that secrete excessive growth hormone (leading to acromegaly) or adrenocorticotropic hormone (ACTH, leading to Cushing's disease). Parretin has many side effects, including inhibition of gallbladder contraction and bile secretion; maintenance therapy may lead to gallstones and elevated serum enzyme and bilirubin levels. Parretin is a synthetic long-acting cyclic peptide with somatostatin-like activity. Parretin activates multiple somatostatin receptors; in vitro studies have shown that its binding affinity for somatostatin receptors 1, 3, and 5 is much higher than that of octreotide, while its binding affinity for somatostatin receptor 2 is comparable. This drug is more potent than somatostatin in inhibiting the release of human growth hormone (HGH), glucagon, and insulin. See also: parretin diaspartate (its active ingredient); parretin pamoate (its active ingredient). Drug Indications For the treatment of Cushing's disease, especially in patients for whom pituitary surgery is ineffective or unsuitable. FDA Label Signifor is indicated for the treatment of adult patients with Cushing's disease who are unsuitable for or have failed surgery. Signifor is also indicated for the treatment of adult patients with acromegaly who are unsuitable for or have failed surgery and whose condition is poorly controlled with other somatostatin analogues. Treatment of acromegaly and pituitary gigantism. Pituitary ACTH oversecretion, pituitary-dependent Cushing's disease, pituitary-dependent hyperadrenocorticism. Mechanism of Action Pasireotide activates multiple somatostatin receptors. In vitro studies have shown that its binding affinity for somatostatin receptors 1, 3, and 5 is significantly higher than that of octreotide, while its binding affinity for somatostatin receptor 2 is comparable. Binding and activation of somatostatin receptors inhibits ACTH secretion, thereby reducing cortisol secretion in patients with Cushing's disease. Furthermore, this drug is more effective than somatostatin in inhibiting the release of human growth hormone (HGH), glucagon, and insulin. Pharmacodynamics: Signifor® is a somatostatin analog that reduces cortisol levels in patients with Cushing's disease. Based on structure-activity relationships, SOM230 (25) was discovered by transferring the functional group of growth hormone release inhibitory factor (SRIF) to a smaller cyclic hexapeptide template through rational drug design. SOM230 is a novel, stable cyclic hexapeptide somatostatin analog with a unique high affinity binding to human somatostatin receptors (subtypes sst1-sst5). SOM230 exhibits potent and sustained inhibition of growth hormone and insulin-like growth factor-1 release and is a promising candidate drug currently undergoing Phase I clinical trials. [1] Pasireotide (SOM230) is a multi-receptor ligand somatostatin analog with high affinity for somatostatin receptor subtypes sst(1,2,3) and sst(5). Pasireotide effectively inhibits the secretion of growth hormone (GH), insulin-like growth factor-I (IGF-I), and adrenocorticotropic hormone (ACTH), suggesting its potential therapeutic efficacy in acromegaly and Cushing's disease. The long-term inhibitory effect of Pasireotide on hormone secretion in animal models and the expression of multiple sst receptors in carcinoid tumors indicate that Pasireotide may have a clinical advantage over octreotide in carcinoid tumor patients. In vitro experiments have observed that Pasireotide has direct and indirect antitumor activities, including sst receptor-mediated apoptosis and anti-angiogenesis, suggesting that Pasireotide may play a role in antitumor therapy. In summary, preclinical evidence and preliminary results from clinical studies suggest that parrete may be a promising new therapy for patients with symptoms, new or persistent acromegaly, of metastatic carcinoid tumors resistant to or refractory to octreotide, and that parrete may become the first targeted drug for Cushing's disease. [3]
In summary, this study is the first to demonstrate the antisecretive, antiproliferative and pro-apoptotic effects of the novel long-acting somatostatin analog SOM230 in a mouse model of insulinoma, and observed that it can improve the overall survival of mice. The enhanced activity spectrum of SOM230 is due to its enhanced activity against four of the five somatostatin receptor subtypes (sstr5, sstr2, sstr3 and sstr1). SOM230 treatment has important clinical significance for unresectable or metastatic insulinomas, especially those that respond poorly to conventional therapies such as octreotide and/or diazoxide. SOM230 treatment may help relieve symptoms and lead to tumor regression. We believe that this novel SOM230 targeted therapy strategy will benefit patients with pancreatic neuroendocrine tumors (PNET). While these data strongly support the efficacy of Pasireotide in this model, we also acknowledge that larger sample studies are needed to advance this new approach to clinical trials. [2] We also investigated the progression of chronic inflammatory histopathological changes after long-term use of Pasireotide. These changes were particularly pronounced after repeated intra-articular injections of the antigen. The current data clearly demonstrate that in this immune-mediated arthritis model, somatostatin receptor (SSTR) agonists can suppress not only acute inflammatory responses but also chronic inflammatory/destructive processes. Somatostatin receptor agonists have attracted much attention in clinical treatment due to their anti-inflammatory (comparable to dexamethasone) and analgesic effects. In fact, significant clinical improvement was observed after treatment with octreotide in a preliminary study of patients with rheumatoid arthritis (RA). Current observations suggest that Pasireotide and octreotide may have similar anti-inflammatory effects; however, Pasireotide is expected to be superior to octreotide in pain control in RA. In addition, somatostatin analogue therapy is considered relatively safe and well-tolerated. Moreover, both octreotide and parretoide have long-acting formulations available for long-term treatment; these formulations only require monthly administration and do not require daily subcutaneous injection. In summary, we provide evidence that the somatostatin receptor agonists octreotide and parretoide have potent anti-inflammatory and analgesic effects. We found that SSTR2 is an important target for the anti-inflammatory effects of somatostatin. Both SSTR2 and SSTR1 can mediate analgesia. Regarding the clinical application of SSTR agonists, pan-SSTR agonists may be considered superior to selective SSTR2 agonists. [4] |
| Molecular Formula |
C60H70N10O11
|
|---|---|
| Molecular Weight |
1107.26
|
| Exact Mass |
1106.522
|
| CAS # |
396091-76-2
|
| Related CAS # |
Pasireotide L-aspartate salt;396091-77-3;Pasireotide pamoate;396091-79-5;Pasireotide;396091-73-9;Pasireotide (diaspartate);1421446-02-7
|
| PubChem CID |
72205932
|
| SequenceShortening |
Cyclo[{4-(NH2-C2H4-NH-CO-O-)Pro}-Phg-{D-Trp}-K-{Tyr(4-Bzl)}-F]
|
| Appearance |
White to off-white solid powder
|
| Hydrogen Bond Donor Count |
10
|
| Hydrogen Bond Acceptor Count |
13
|
| Rotatable Bond Count |
18
|
| Heavy Atom Count |
81
|
| Complexity |
1970
|
| Defined Atom Stereocenter Count |
7
|
| SMILES |
CC(=O)O.C1[C@H](CN2[C@@H]1C(=O)N[C@H](C(=O)N[C@@H](C(=O)N[C@H](C(=O)N[C@H](C(=O)N[C@H](C2=O)CC3=CC=CC=C3)CC4=CC=C(C=C4)OCC5=CC=CC=C5)CCCCN)CC6=CNC7=CC=CC=C76)C8=CC=CC=C8)OC(=O)NCCN
|
| InChi Key |
WFKFNBBHVLMWQH-QKXVGOHISA-N
|
| InChi Code |
InChI=1S/C58H66N10O9.C2H4O2/c59-27-13-12-22-46-52(69)64-47(30-38-23-25-42(26-24-38)76-36-39-16-6-2-7-17-39)53(70)66-49(31-37-14-4-1-5-15-37)57(74)68-35-43(77-58(75)61-29-28-60)33-50(68)55(72)67-51(40-18-8-3-9-19-40)56(73)65-48(54(71)63-46)32-41-34-62-45-21-11-10-20-44(41)45;1-2(3)4/h1-11,14-21,23-26,34,43,46-51,62H,12-13,22,27-33,35-36,59-60H2,(H,61,75)(H,63,71)(H,64,69)(H,65,73)(H,66,70)(H,67,72);1H3,(H,3,4)/t43-,46+,47+,48-,49+,50+,51+;/m1./s1
|
| Chemical Name |
(3S,6R,9S,12S,15S,19R,20aS)-6-((1H-indol-3-yl)methyl)-9-(4-aminobutyl)-15-benzyl-12-(4-(benzyloxy)benzyl)-1,4,7,10,13,16-hexaoxo-3-phenylicosahydropyrrolo[1,2-a][1,4,7,10,13,16]hexaazacyclooctadecin-19-yl (2-aminoethyl)carbamate acetate
|
| Synonyms |
SOM 230; SOM-230; Pasireotide acetate; 396091-76-2; Pasireotide acetate salt [MI]; UNII-662X0VFR9L; 662X0VFR9L; Cyclo((2S)-2-phenylglycyl-D-tryptophyl-L-lysyl-O-(phenylmethyl)-L-tyrosyl-L-phenylalanyl-(4R)-4-((((2-aminoethyl)amino)carbonyl)oxy)-L-prolyl), monoacetate; Pasireotide acetate salt; Pasireotide (acetate); SOM230; trade name: Signifor; Signifor LAR.
|
| HS Tariff Code |
2934.99.9001
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: Please store this product in a sealed and protected environment (e.g. under nitrogen), avoid exposure to moisture and light. |
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
DMSO : ~100 mg/mL (~90.31 mM)
H2O : ~1 mg/mL (~0.90 mM) |
|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: 2.5 mg/mL (2.26 mM) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), suspension solution; with sonication.
For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.5 mg/mL (2.26 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. View More
Solubility in Formulation 3: ≥ 2.5 mg/mL (2.26 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. Solubility in Formulation 4: 2 mg/mL (1.81 mM) in PBS (add these co-solvents sequentially from left to right, and one by one), clear solution; with ultrasonication. |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 0.9031 mL | 4.5157 mL | 9.0313 mL | |
| 5 mM | 0.1806 mL | 0.9031 mL | 1.8063 mL | |
| 10 mM | 0.0903 mL | 0.4516 mL | 0.9031 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
| NCT Number | Recruitment | interventions | Conditions | Sponsor/Collaborators | Start Date | Phases |
| NCT01329289 | Withdrawn | Drug: SOM230 Drug: Bortezomib Drug: Dexamethasone |
Multiple Myeloma Multiple Myeloma in Relapse |
University of Pittsburgh | 2011-12 | Phase 2 |
|
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved





























 COA
COA