| Size | Price | Stock | Qty |
|---|---|---|---|
| 250mg |
|
||
| 500mg |
|
||
| Other Sizes |
































| ln Vitro |
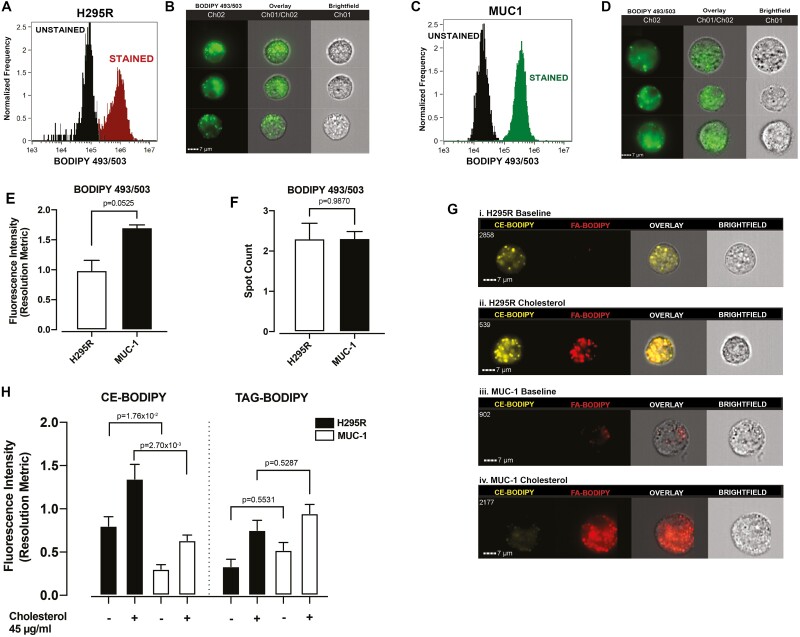
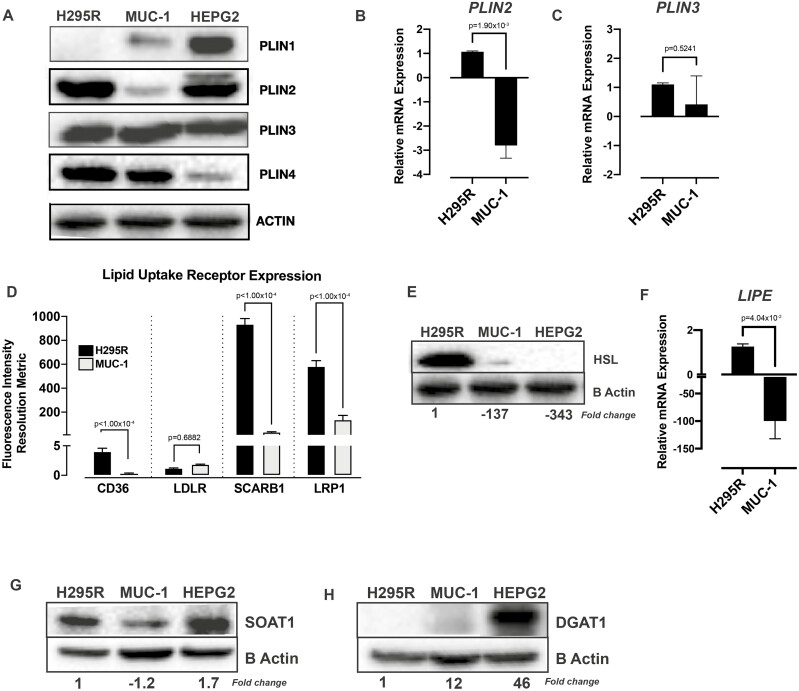
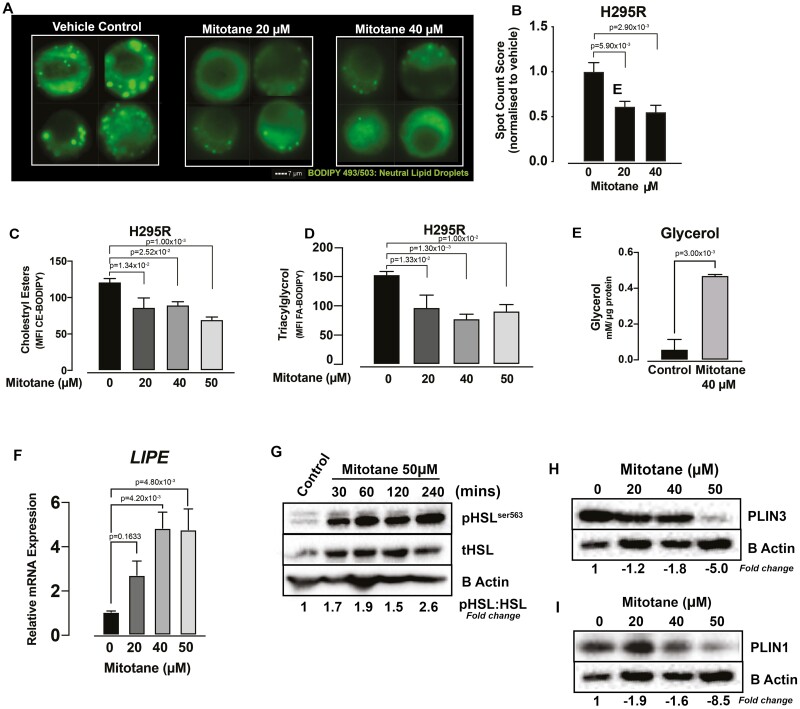
The growth of H295R cells is considerably inhibited by mitotane (1 nM-100 μM; 6 days) [1]. In TαT1 cells, mitotane (10-100 μM; 6 or 48 hours) dramatically enhances caspase 3/7 activity in the range of 60 μM to 80 μM, while decreasing TαT1 cell viability in a time- and dose-dependent manner. Because caspase 3/7 activity was considerably raised from 40 μM to 100 μM by TSH and TSH β-subunit mRNA expression. In a dose-dependent manner, mitotane (1-30 μM; 24 hours; HepG2) stimulates the transcription of the CYP3A4 and CYP2B6 genes [3]. In HepaRG, mitotane (20 and 40 μM; 6 h) dramatically decreased the amount of neutral lipid droplets per cell and also considerably decreased triglycerol-labeled lipid droplets, which in turn decreased PLIN1 and PLIN3 expression levels [4].
|
|---|---|
| ln Vivo |
Early on after H295R cell seeding, mitotane (440 mg/kg; ip or po, 5 days per week for 7 weeks) dramatically decreases xenograft volume [1].
|
| Cell Assay |
Cell Proliferation Assay[1]
Cell Types: H295R Cell Tested Concentrations: 1 nM-100 μM Incubation Duration: 6 days Experimental Results: H295R cells Dramatically diminished proliferation with an IC50 of 22.8 μM. Cell viability assay[2] Cell Types: TαT1 Cell Tested Concentrations: 10, 40, 60, 80 and 100 μM Incubation Duration: 6 or 48 hrs (hours) Experimental Results: No change in cell viability at 10-80 μM, but significant (P < 0.01 ), cell viability diminished (-56%) at 100 μM after 6 hrs (hours) of incubation. Cell viability was not altered at 10-60 μM, whereas at 60 μM (-31%; P < 0.05), 80 μM (-53%; P < 0.01), and 100 μM (-75.5%; P < 0.01) Dramatically diminished. P < 0.01), after 48 hrs (hours) of incubation. RT-PCR[3] Cell Types: HepaRG cells and human hepatocytes Tested Concentrations: 0.1, 1, 10, 20, 30 or 40 μM Incubation Duration: 24 or 48 hrs (hours) Experimental Results: Increased mRNA levels of CYP3A4 and CYP2B6. Western Blot Analysis[4] Cell Types: H295R Tested Concentrations: 20, 40 and 50 μM Incubation Duration: 6 hrs (hours) Experimental Results: diminished expression levels of PLIN1 and PLIN3. |
| Animal Protocol |
Animal/Disease Models: NOD/SCID/γcnull mice (4 weeks old; 6 × 106 H295R cells were inoculated subcutaneously (sc) (sc) into the right flank) [1]
Doses: 440 mg/kg Route of Administration: ip or po; 5 days a week , continued for 7 weeks. Experimental Results: At an early time point (day 13) after H295R cell seeding, xenograft volume was Dramatically diminished. The effect of oral mitotane treatment became insignificant on day 20 after H295R cell inoculation, whereas the effect of intraperitonealmitotane continued until day 34. |
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion
The bioavailability of mitotane via oral administration is 40%. Approximately 10% of the administered dose is excreted in the urine as water-soluble metabolites, and another 1% to 17% of metabolites are excreted via bile. Mitotane is widely distributed and present in most tissues of the body. Adipose tissue is its primary site of distribution. Clinical studies have shown that approximately 40% of mitotane is absorbed after oral administration. After a daily dose of 5 to 15 grams, the unchanged drug concentration in the blood is 10 to 90 μg/mL, and the metabolite concentration is 30 to 50 μg/mL. Mitotane remains detectable in plasma for 6 to 9 weeks after discontinuation of the drug. Although the drug is present in all tissues, adipose tissue is its primary storage site. Peak plasma concentrations of mitotane occur 3–5 hours after a single oral dose, and distribution of the drug between plasma and tissues is completed within 12 hours. In a study of patients with adrenocortical carcinoma, patients received 5-15 g of mitotane orally daily, resulting in serum mitotane concentrations of 7-90 μg/mL and serum mitotane metabolite concentrations of 29-54 μg/mL. Serum concentrations of mitotane and its metabolites appeared to plateau after approximately 8 weeks of continuous mitotane treatment and were generally unrelated to the drug's therapeutic or toxic effects; however, some data suggest that tumor regression in adrenocortical carcinoma patients was associated with serum mitotane concentrations above 14 μg/mL, while central nervous system adverse reactions were associated with serum concentrations above 20 μg/mL. Mitotane and its metabolites are distributed in almost all body tissues, with adipose tissue being the primary storage site; they do not selectively accumulate in the adrenal glands. The sustained plasma concentrations of mitotane and its metabolites after discontinuation of mitotane treatment are likely due to their slow release from adipose tissue and other tissues. Although unchanged mitotane was not detected in cerebrospinal fluid (CSF), trace amounts of mitotane metabolites were detected in CSF. It is currently unclear whether mitotane or its metabolites can cross the placenta or be distributed into breast milk. For more complete data on the absorption, distribution, and excretion of mitotane (11 metabolites), please visit the HSDB record page. Mitotane undergoes extensive metabolism—including intrahepatic and extrahepatic metabolism—and is not excreted unchanged in bile or urine. The major circulating metabolite of mitotane is 1,1-(o,p'-dichlorodiphenyl)acetic acid (o,p'-DDA). In rabbits and humans, o,p'-dichlorodiphenylacetic acid has been identified as the major urinary metabolite of mitotane. Following oral administration of mitotane, the metabolite o,p'-dichlorodiphenylacetic acid and its monohydroxylated and dihydroxylated derivatives appear in urine and feces. The unsaturated metabolite o,p'-DDE has been observed in human plasma and tissues. Urine samples were collected from four patients with Cushing's syndrome who received o-,p'-DDD treatment. Methyl thio group-containing metabolites, as well as other o-,p'-DDD metabolites, were detected in the urine samples by gas chromatography-mass spectrometry. The peak intensities of these methyl thio group-containing metabolites in the gas chromatograms were lower than those of other o-,p'-DDD-derived metabolites. The biological significance of the pathways leading to the formation of these methyl thio group-containing metabolites is currently unclear. ... Mitotan is primarily metabolized in the liver and other tissues to o-,p'-dichlorodiphenylethylene and acetate derivatives; small amounts of these derivatives appear to undergo aromatic hydroxylation and glycine conjugation. For more complete metabolite/metabolite data on mitotane (6 metabolites in total), please visit the HSDB record page. After absorption in the stomach and intestines, DDD enters the lymphatic system and is transported throughout the body, eventually integrating into adipose tissue. The metabolism of DDD is primarily carried out by cytochrome P-450 enzymes in the liver and kidneys. Its metabolites, primarily DDA (bis(p-chlorophenyl)acetic acid), are excreted in the urine. (L85) Elimination pathway: Some metabolites (1%-17%) are excreted in bile, while the remainder are stored in tissues. Half-life: 18-159 days Biological half-life The terminal plasma half-life of mitotane is 18 to 159 days, with a median of 53 days. It has been reported that the plasma elimination half-life of mitotane is 18-159 days. |
| Toxicity/Toxicokinetics |
Toxicity Summary
DDD toxicity occurs through at least four mechanisms, possibly all simultaneously. DDD reduces transmembrane potassium transport. DDD inhibits the inactivation of voltage-gated sodium channels. These channels normally activate (open) but inactivate (close) slowly, interfering with the active transport of sodium ions out of nerve axons during repolarization, leading to neuronal hyperexcitability. DDD inhibits neuronal adenosine triphosphatases (ATPases), particularly Na+K+-ATPase and Ca2+-ATPase, which play crucial roles in neuronal repolarization. DDD also inhibits the ability of calmodulin (a calcium mediator) in neurons to transport calcium ions, which are essential for neurotransmitter release. All these inhibited functions reduce the rate of depolarization and increase the sensitivity of neurons to weak stimuli that would not elicit a response in fully depolarized neurons. DDD is also thought to have adverse effects on the reproductive system by mimicking endogenous hormones and binding to estrogen and androgen receptors. (T10, L85) Hepatotoxicity Up to half of patients receiving standard doses of mitotane experience elevated serum transaminases, but elevations exceeding 5 times the upper limit of normal are uncommon ( Probability score: E (Unproven but suspected rare cause of clinically significant liver injury)). Protein binding rate 6% Toxicity data LD50: 113 mg/kg (oral, rat) (L138) Drug Interactions Because mitotane alters metabolism, higher doses of corticosteroids, glucocorticoids, and mineralocorticoids may be required to treat adrenal insufficiency. Concomitant use of central nervous system depressants and mitotane may produce additive central nervous system depressant effects. Side Effects. Mitotane may inhibit the adrenal response to adrenocorticotropic hormone (ACTH); this may interfere with the therapeutic effect of ACTH. Mitotane has been reported to accelerate warfarin metabolism through the induction of hepatic microsomal enzymes, leading to an increased warfarin dose requirement. Therefore, physicians should closely monitor patients taking coumarin anticoagulants for changes in anticoagulant dose requirements when mitotane is used. Furthermore, mitotane should be used with caution in patients taking other medications that are susceptible to hepatic enzyme induction. |
| References |
[1]. Doghman M, et al. Lack of long-lasting effects of mitotane adjuvant therapy in a mouse xenograft model of adrenocortical carcinoma. Mol Cell Endocrinol. 2013 Dec 5;381(1-2):66-9.
[2]. Zatelli MC, et al. Therapeutic concentrations of mitotane (o,p'-DDD) inhibit thyrotroph cell viability and TSH expression and secretion in a mouse cell line model. Endocrinology. 2010 Jun;151(6):2453-61. [3]. Takeshita A, Igarashi-Migitaka J, Koibuchi N, Mitotane induces CYP3A4 expression via activation of the steroid and xenobiotic receptor. J Endocrinol. 2013 Feb 15;216(3):297-305. [4]. Warde KM, et al. Mitotane Targets Lipid Droplets to Induce Lipolysis in Adrenocortical Carcinoma. Endocrinology. 2022 Sep 1;163(9):bqac102. |
| Additional Infomation |
Therapeutic Uses
Mitotan is an anti-tumor drug and a hormonal agent. It is indicated for the treatment of unresectable functional and non-functional adrenocortical carcinoma. /Included in the US product label/ Mitotan is also used to treat Cushing's syndrome. /Not included in the US or Canadian product label/ A study evaluating the efficacy of mitotane in treating adrenocortical carcinoma included 88 patients (mean age 46 years); 80 patients underwent surgery, and 59 patients received oral mitotane capsules concurrently. The mean initial dose was 10 g/day, the mean maintenance dose was 7 g/day, and the mean treatment duration was 10.5 months. The median disease-free survival after surgery was 12.1 months. 82% of patients developed tumor metastases, the most common sites being the lungs, liver, and adjacent organs. The median survival was 14.5 months, and the 5-year survival rate was 22%. Age over 40 years and the presence of metastases at diagnosis were the only recognized factors for poor prognosis. Mitotan controlled hormone secretion in 75% of patients. In 8 patients treated with mitotane, tumors partially regressed, but the drug had no significant effect on survival. The conclusion is that adrenocortical carcinoma has a poor prognosis; mitotane treatment may provide transient benefits, particularly in controlling endocrine symptoms. Drug Warning /Black Box Warning/ Warning: Lysodren (mitotane tablets, USP) should be used under the supervision of a qualified physician experienced in the use of chemotherapy drugs for cancer. Because the primary action of Lysodren is adrenal suppression, it should be temporarily discontinued immediately after shock or severe trauma. In such cases, exogenous steroids should be administered, as adrenal insufficiency may not immediately initiate steroid secretion. …Between 1999 and 2005, 17 consecutive patients who underwent radical resection of adrenocortical carcinoma (ACC) and received mitotane treatment underwent physical examination, routine laboratory tests, mitotane concentration monitoring, and hormone level monitoring every 3 months from baseline until ACC recurrence or the end of the study (December 2007). Mitopanol toxicity grading was performed using the NCI CTCAE standard. All biochemical indicators were measured at our center, and plasma mitotane concentrations were determined using our in-house high-performance liquid chromatography (HPLC) method. All patients achieved mitotane concentrations >14 mg/L, and none required permanent discontinuation due to toxicity; in 14 patients, mitotane concentrations continued to rise after gradual dose reduction. All patients experienced side effects, which were manageable with palliative care and adjustments to hormone replacement therapy. Mitopanol affects adrenal steroid production, with a more significant inhibitory effect on cortisol and dehydroepiandrosterone sulfate (DHEAS) than on aldosterone. Mitopanol can cause thyroid dysfunction, similar to central hypothyroidism; or suppress testosterone secretion in male patients. Differences in salivary and serum cortisol levels, as well as total and free testosterone levels, are due to mitotane-induced increases in hormone-binding proteins, complicating the interpretation of hormone measurements. …Researchers prospectively studied seven patients with adrenocortical carcinoma treated with mitotane. Platelet counts, bleeding time, and overall coagulation parameters were measured before initiation of mitotane treatment and at 1 week and 2 weeks or longer after treatment. All patients had normal bleeding times before treatment. Six patients had prolonged bleeding times (245–555 seconds). Four patients exhibited platelet aggregation responses consistent with aspirin-like defects. The conclusion was that mitotane may cause clinically significant platelet dysfunction. Gastrointestinal disturbances (anorexia, nausea, vomiting, and diarrhea) occurred in 80% of patients, and these symptoms are often dose-limiting factors. Central nervous system side effects (drowsiness and somnolence, 25%; dizziness or vertigo, 15%) occurred in approximately 40% of patients. Dermatitis occurred in approximately 15% of patients. For more complete data on mitotane (28 total), please visit the HSDB record page. Pharmacodynamics Mitotan administration alters peripheral steroid metabolism, leading to decreased plasma 17-hydroxycorticosteroid levels and increased 6-β-hydroxycorticosteroid levels, while corticosteroid levels remain normal. |
| Molecular Formula |
C14H10CL4
|
|---|---|
| Molecular Weight |
320.0412
|
| Exact Mass |
317.953
|
| CAS # |
53-19-0
|
| Related CAS # |
Mitotane-13C6;1261396-21-7;Mitotane-d8;2673270-14-7
|
| PubChem CID |
4211
|
| Appearance |
Crystals from pentane or methanol
|
| Density |
1.4±0.1 g/cm3
|
| Boiling Point |
398.9±37.0 °C at 760 mmHg
|
| Melting Point |
77-78 °C(lit.)
|
| Flash Point |
194.2±23.9 °C
|
| Vapour Pressure |
0.0±0.9 mmHg at 25°C
|
| Index of Refraction |
1.599
|
| LogP |
5.39
|
| Hydrogen Bond Donor Count |
0
|
| Hydrogen Bond Acceptor Count |
0
|
| Rotatable Bond Count |
3
|
| Heavy Atom Count |
18
|
| Complexity |
248
|
| Defined Atom Stereocenter Count |
0
|
| SMILES |
ClC([H])(C([H])(C1=C([H])C([H])=C([H])C([H])=C1Cl)C1C([H])=C([H])C(=C([H])C=1[H])Cl)Cl
|
| InChi Key |
JWBOIMRXGHLCPP-UHFFFAOYSA-N
|
| InChi Code |
InChI=1S/C14H10Cl4/c15-10-7-5-9(6-8-10)13(14(17)18)11-3-1-2-4-12(11)16/h1-8,13-14H
|
| Chemical Name |
1-chloro-2-[2,2-dichloro-1-(4-chlorophenyl)ethyl]benzene
|
| HS Tariff Code |
2934.99.9001
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
DMSO : ≥ 100 mg/mL (~312.46 mM)
|
|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.5 mg/mL (7.81 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution.
For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: 2.5 mg/mL (7.81 mM) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), suspension solution; with ultrasonication. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. View More
Solubility in Formulation 3: ≥ 2.5 mg/mL (7.81 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 3.1246 mL | 15.6230 mL | 31.2461 mL | |
| 5 mM | 0.6249 mL | 3.1246 mL | 6.2492 mL | |
| 10 mM | 0.3125 mL | 1.5623 mL | 3.1246 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
|
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved