| Size | Price | Stock | Qty |
|---|---|---|---|
| 1g |
|
||
| 5g |
|
||
| Other Sizes |
































| ln Vitro |
Biotin exhibits a greater affinity for breast cancer (T47D) cells compared to normal mammary epithelial (MCF-12A) cells, as seen by Kms values of 9.24 μM and 53.1 μM, respectively [4]. T47D cells have a dose-dependent uptake of biotin (0.09-100 μM; 0-70 min), with a Vmax of 27.34 pmol/mg protein/min [4]. Cell adhesion is decreased and 7β-OHC (50 µM)-induced cell death is partially restored by biotin (1–1000 nM; 24 hours) [5].
|
|---|---|
| ln Vivo |
In rats given streptozotocin (150 mg/kg; intraperitoneal) to produce diabetes, biotin (15 mg/kg/d; oral; 12 days) reduces nephrotoxicity [6]. Fish given insufficient levels of biotin (0.012 mg/kg/d; po; 70 d) had impaired immunological activity in the brain, spleen, and skin [7].
|
| Cell Assay |
Cell Viability Assay [5]
Cell Types: Mouse Oligodendrocytes 158N Cell Tested Concentrations: 1, 10, 100, 1000 nM Incubation Duration: 24 hrs (hours) Experimental Results: Shows cytoprotective effect and prevents 7β-hydroxycholesterol-induced redox State destruction. Improve the attenuation of oxidative stress, mitochondrial dysfunction, and lipid metabolism changes. |
| Animal Protocol |
Animal/Disease Models: Streptozotocin-induced male Swiss albino mice (25±2 g) [6]
Doses: 15 mg/kg/d Route of Administration: po (oral gavage); 12-day Experimental Results: Improved histopathological results, Includes distorted glomeruli, inflammatory cells, and macrophages, and reduces the acrylate response to oxidative damage. Animal/Disease Models: grass carp (117±0.5 g) [7] Doses: 0.012, 0.110, 0.214, 0.311, 0.427 and 0.518 mg/kg Route of Administration: po (oral gavage); 70-day Experimental Results: Lysozyme (LZ) and acid phosphatase (ACP) activity is diminished, and the levels of complement 3 (C3), C4 and immunoglobulin M (IgM) are diminished. Decreases the mRNA levels of antimicrobial substances. It partially increases the mRNA levels of pro-inflammatory cytokines and tumor necrosis factor, partially reduces the levels of anti-inflammatory IL-4/13A, IL-10, IL-11 and TGF-β1 mRNA, and partially interacts with target of rapamycin (TOR) signaling. Conduction related. |
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion
Systemic Absorption - Approximately 50% The gut can access biotin from multiple sources: diet, biotin supplements, and biotin synthesized by E. coli. Dietary biotin exists in both free and protein-bound forms. Protein-bound biotin is digested by proteases and peptidases into biotin-containing oligopeptides and biocytin (ε-N-biotinyl-L-lysine). Biocytin and biotin-containing oligopeptides are then converted to biotin by biotinylate enzymes. Both dietary and supplemental biotin are effectively absorbed by the small intestine. At dietary doses of biotin, biotin appears to be transported to intestinal cells via sodium-dependent carriers. At higher doses of biotin, absorption appears to occur via passive diffusion. Absorption of biotin produced by the colonic microbiota appears to occur via carrier-mediated processes in the proximal colon. Excretion: Primarily excreted in urine. Protein Binding: Primarily bound to plasma proteins. Absorption: Approximately 50%. For more complete data on the absorption, distribution, and excretion of biotin (32 types), please visit the HSDB records page. Biotin is excreted in urine as biotin, dinorbiotin, biotin sulfoxide, biotin sulfone, dinorbiotin methyl ketone, and tetramethylenebiotin-1-sulfoxide. Biotin is metabolized into several different metabolites, including dinorbiotin, biotin sulfoxide, biotin sulfone, dinorbiotin methyl ketone, and tetramethylenebiotin-1-sulfoxide. Tetranorbiotin-1-sulfoxide. Over 95% of biotin exists in free form in the skimmed fraction of human breast milk. Biotin concentrations vary considerably in some women, sometimes by one to two orders of magnitude higher than in serum, suggesting the presence of a transport system that transfers biotin into breast milk. The biotin metabolite dinorbiotin accounts for approximately 50%. In early and transitional human milk, biotin sulfoxide, a biotin metabolite, accounts for approximately 10% of the total biotin and its metabolites. Biotin concentration increases as breast milk matures postpartum, but by 5 weeks postpartum, the concentrations of dinorbiotin and biotin sulfoxide are 25% and 8%, respectively. Current research provides no evidence of soluble biotin-binding proteins or any other mechanism that can capture biotin in human milk. Biotin accounts for approximately half of all avidin-binding substances in human serum and urine at molar concentrations. Biotinycin, dinorbiotin, dinorbiotin methyl ketone, biotin sulfoxide, and biotin sulfone constitute the majority of biotin metabolism. Anticonvulsant drugs and pregnancy can accelerate biotin metabolism in some individuals, thereby increasing the ratio of biotin metabolites to biotin in urine. Besides being absorbed by carboxylases or excreted unchanged, another metabolic pathway for biotin is its breakdown into inactive metabolites before excretion in urine. Approximately half of biotin undergoes metabolism before excretion. Two main biotin catabolism pathways have been identified in mammals. In the first pathway, the valerate side chain of biotin is degraded via β-oxidation. This leads to the formation of dinorbiotin, tetranorbiotin, and related intermediates known to arise from fatty acid β-oxidation. The cellular localization of biotin β-oxidation is not yet fully understood. The non-enzymatic decarboxylation of unstable β-ketobiotin and β-ketodinorbiotin produces dinorbiotin methyl ketone and tetranorbiotin methyl ketone, which are found in urine. In the second pathway, the sulfur atom on the biotin thiophene ring is oxidized to produce biotin L-sulfoxide, biotin D-sulfoxide, and biotin sulfone. The oxidation of the cyclic sulfur atom and the β-oxidation of the side chain work together to produce metabolites such as dinorbiotin sulfone. In mammals, the amount of carbon dioxide and urea released during biotin ring degradation is minimal. |
| Toxicity/Toxicokinetics |
Toxicity Summary
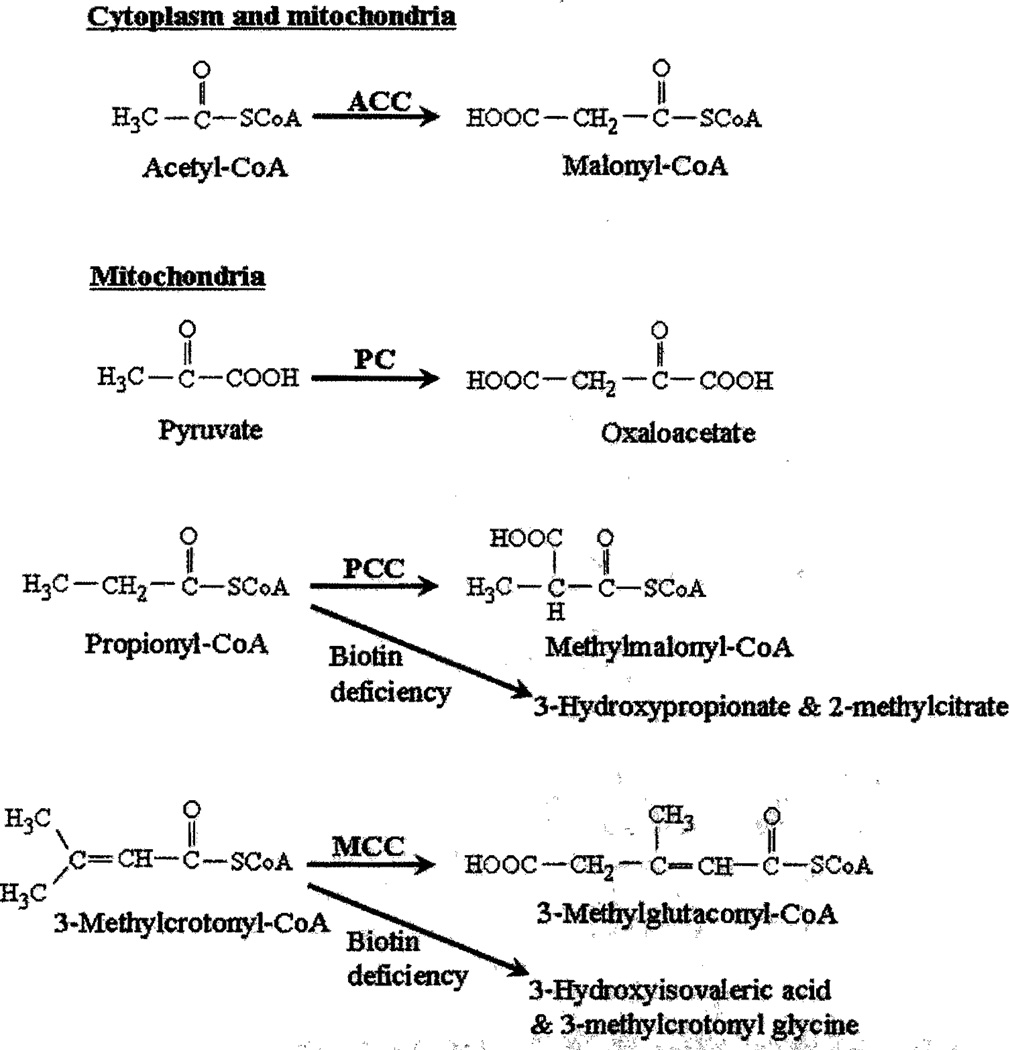
Biotin is essential for the normal functioning of enzymes that transport carboxyl units and fix carbon dioxide, and is also necessary for a variety of metabolic functions, including gluconeogenesis, lipogenesis, fatty acid biosynthesis, propionic acid metabolism, and branched-chain amino acid catabolism. Interactions Carbamazepine, phenytoin, and phenobarbital can accelerate biotin metabolism and may lead to decreased biotin levels. Long-term use of carbamazepine, phenytoin sodium, phenobarbital, and primidone is associated with decreased plasma biotin concentrations. Antibiotic use may reduce the contribution of coliform bacteria to biotin in the body. Holzmann rats were mated in groups, and pregnant female rats were subcutaneously injected with 100 mg D(+)-biotin (dissolved in 0.2 mL 0.1 N NaOH solution)/kg body weight on days 0 and 1 of gestation. Nine animals received only biotin injections. Seven animals received subcutaneous injections of biotin and 0.1 μg of 17(β)-estradiol (dissolved in 0.05 mL olive oil) from day 5 to day 20 of gestation, while the other seven animals received subcutaneous injections of biotin and 4 mg of progesterone (dissolved in 0.2 mL olive oil) from day 5 to day 20 of gestation. Nine pregnant animals received no treatment and served as a negative control group. Three groups of six non-pregnant animals were also included, administered the same way as the pregnant animals, serving as a non-pregnant treatment control group. All animals were sacrificed and examined on day 21 of gestation. In eight of the nine rats treated with biotin alone, complete fetal resorption occurred; however, concurrent estrogen or progesterone treatment prevented fetal resorption. Compared to the control group, the animals receiving biotin combined with estrogen or progesterone treatment showed decreased fetal and placental weights, but the differences were not statistically significant. Biotin caused a decrease in body weight in both pregnant and non-pregnant animals; the body weight of pregnant animals treated with biotin in combination with progesterone was similar to that of the untreated pregnant control group, while the body weight of pregnant animals treated with biotin in combination with estrogen increased. The uterine weight of pregnant animals given biotin and estrogen was similar to that of the untreated pregnant control group, while the uterine weight of animals given biotin and progesterone was significantly reduced. Holzmann rats were mated in groups, and pregnant females were subcutaneously injected with 100 mg D(+)-biotin per kilogram of body weight (dissolved in 0.2 mL of 0.1N NaOH solution) on days 13 and 14 of gestation. Eleven animals received only biotin, seven animals received subcutaneous biotin and 0.1 μg 17β-estradiol (dissolved in 0.05 mL of olive oil) until day 20 of gestation, and seven animals received subcutaneous biotin and 4 mg progesterone (dissolved in 0.2 mL of olive oil) until day 20 of gestation. Nine pregnant animals received no treatment and served as a negative control group. Animals were sacrificed and examined on day 21 of gestation. Two of the eleven animals treated with biotin alone experienced embryo resorption. Compared to the control group, the remaining nine animals in this group showed significantly lower maternal body weight, as well as fetal, uterine, and placental weights. The maternal body weight, as well as fetal, uterine, and placental weights, of animals treated with biotin and estrogen were similar to those of the control group; the maternal body weight and uterine weight of animals treated with biotin and progesterone were also similar to those of the control group. Liver and ovarian weights were similar in both the experimental and control groups. For more complete data on interactions of biotin (6 items), please visit the HSDB record page. Non-human toxicity values Oral LD50 in rats >1.45 mmol/kg Oral LD50 in mice >10 g/kg |
| References | |
| Additional Infomation |
Therapeutic Uses
B vitamins are indicated for the prevention and treatment of vitamin B deficiency. Vitamin B deficiency can be caused by malnutrition or malabsorption, but it is not common in healthy individuals with a balanced diet. Deficiency of a single B vitamin is rare, as dietary inadequacy usually leads to deficiencies in multiple vitamins. For the prevention of biotin deficiency, dietary improvement is recommended rather than biotin supplementation. For the treatment of biotin deficiency, biotin supplementation is recommended. /US product label contains/ High doses of biotin…are used to treat infantile seborrheic dermatitis and individuals with biotin-dependent enzyme gene mutations. Patients receiving long-term parenteral nutrition should take vitamin preparations containing biotin. (Veterinary): Biotin is used as a feed additive for poultry and pigs. Biotin is used to treat congenital metabolic defects that respond to biotin, including polycarboxylase synthase deficiency and biotinase deficiency. Polycarboxylase deficiency is the most common cause of neonatal polycarboxylase deficiency. Biotinase deficiency is the most common cause of late-onset polycarboxylase deficiency. For more complete data on the therapeutic uses of biotin (11 types), please visit the HSDB record page. Drug Warnings Biotin deficiency (which may be caused by feeding uncooked egg whites or a lack of biotin in the diet) can cause hair loss and characteristic scaly erythematous dermatitis around the body cavity in infants, children, and adults. In adults, long-term biotin deficiency can lead to depression, lethargy, hallucinations, and paresthesia in the extremities. Biotin has not been shown to be effective in treating acne, seborrheic dermatitis, or hair loss. Biotin is a water-soluble B vitamin composed of a urea ring and a tetrahydrothiophene ring fused together, with a valeric acid substituent attached to one carbon atom. Biotin is involved in cell growth, fatty acid synthesis, and the metabolism of fats and amino acids. It plays a role in the tricarboxylic acid cycle (the process of releasing energy from food). Biotin not only helps with various metabolic chemical transformations but also with the transfer of carbon dioxide. Biotin also helps maintain stable blood sugar levels. Biotin is often recommended for strong hair and nails. Therefore, biotin is widely used in many hair and skin care cosmetics and health products. Biotin deficiency is a rare nutritional disorder caused by insufficient biotin in the body. Early symptoms of biotin deficiency include: dry skin, seborrheic dermatitis, fungal infections, rashes (including erythematous macules around the face), fine and brittle hair, and hair loss or complete alopecia. If left untreated, neurological symptoms may occur, including mild depression (which may develop into extreme fatigue, eventually leading to drowsiness), altered mental status, generalized muscle pain (myalgia), hyperesthesia, and paresthesia. Treatment for biotin deficiency is simple: just take biotin supplements. In infants, biotin deficiency can cause a condition called seborrheic dermatitis or "cradle cap." Biotin deficiency is extremely rare in adults, but if it occurs, it can cause anemia, depression, hair loss, high blood sugar, muscle pain, nausea, loss of appetite, and inflammation of the mucous membranes. |
| Molecular Formula |
C10H16N2O3S
|
|---|---|
| Molecular Weight |
244.3106
|
| Exact Mass |
244.088
|
| CAS # |
58-85-5
|
| Related CAS # |
Biotin-d2-1;1217481-41-8;Biotin sodium;56085-82-6;rel-Biotin-d4;1217850-77-5;Biotin-d2
|
| PubChem CID |
171548
|
| Appearance |
White to off-white solid powder
|
| Density |
1.6±0.1 g/cm3
|
| Boiling Point |
492.3±55.0 °C at 760 mmHg
|
| Melting Point |
231-233 °C(lit.)
|
| Flash Point |
251.5±31.5 °C
|
| Vapour Pressure |
0.0±2.8 mmHg at 25°C
|
| Index of Refraction |
1.717
|
| LogP |
0.03
|
| Hydrogen Bond Donor Count |
3
|
| Hydrogen Bond Acceptor Count |
4
|
| Rotatable Bond Count |
5
|
| Heavy Atom Count |
16
|
| Complexity |
298
|
| Defined Atom Stereocenter Count |
3
|
| SMILES |
C1[C@H]2[C@@H]([C@@H](S1)CCCCC(=O)O)NC(=O)N2
|
| InChi Key |
YBJHBAHKTGYVGT-ZKWXMUAHSA-N
|
| InChi Code |
InChI=1S/C10H16N2O3S/c13-8(14)4-2-1-3-7-9-6(5-16-7)11-10(15)12-9/h6-7,9H,1-5H2,(H,13,14)(H2,11,12,15)/t6-,7-,9-/m0/s1
|
| Chemical Name |
5-[(3aS,4S,6aR)-2-oxo-1,3,3a,4,6,6a-hexahydrothieno[3,4-d]imidazol-4-yl]pentanoic acid
|
| HS Tariff Code |
2934.99.9001
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
DMSO : ~100 mg/mL (~409.32 mM)
|
|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 2.5 mg/mL (10.23 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution.
For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 400 μL PEG300 and mix evenly; then add 50 μL Tween-80 to the above solution and mix evenly; then add 450 μL normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 2.5 mg/mL (10.23 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 25.0 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. View More
Solubility in Formulation 3: ≥ 2.5 mg/mL (10.23 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. Solubility in Formulation 4: 1.96 mg/mL (8.02 mM) in PBS (add these co-solvents sequentially from left to right, and one by one), clear solution; with ultrasonication (<60°C). |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 4.0932 mL | 20.4658 mL | 40.9316 mL | |
| 5 mM | 0.8186 mL | 4.0932 mL | 8.1863 mL | |
| 10 mM | 0.4093 mL | 2.0466 mL | 4.0932 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved