| Size | Price | Stock | Qty |
|---|---|---|---|
| 250mg |
|
||
| 500mg |
|
||
| 1g |
|
||
| 5g |
|
||
| Other Sizes |
| ln Vitro |
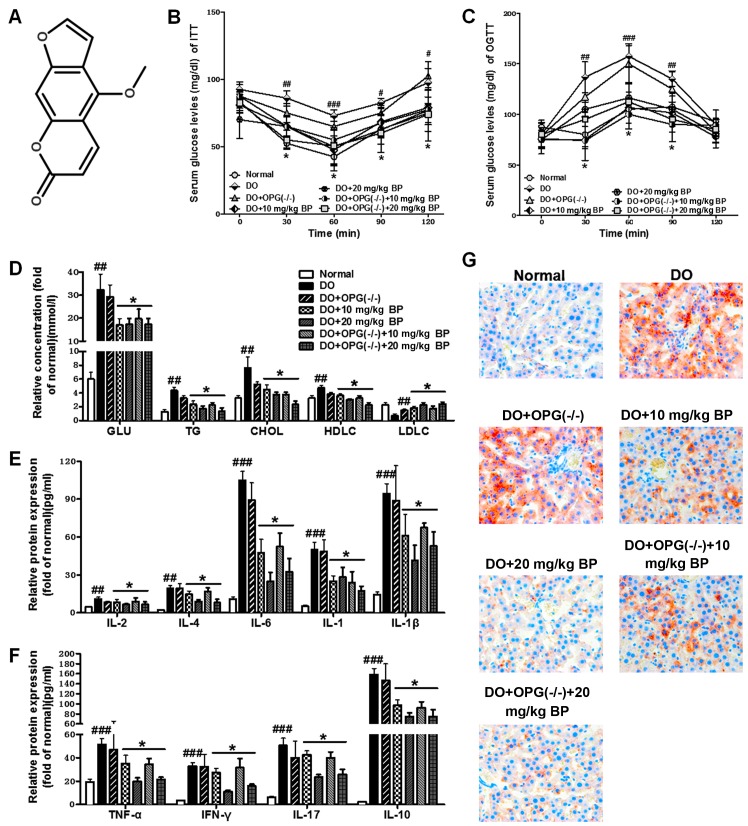
Bergamotene (5-methoxypsoralen, 5-MOP) concentrations ranged from 0.05 to 25 mM, however there was no change in N-acetyltransferase (NAT) activity in SC-M1 cells between these levels. There was a noticeable dose-dependent effect (r = 0.5687). In COLO 205 cells, bergamotenol at low concentrations (0.05 mM and 0.5 mM) boosted NAT activity, but at high levels (50 mM), it decreased. At our experimental concentration (r=0.8912), bergamotene exhibited a dose-dependent effect on COLO 205 cells: a high dose (50 mM) exhibited a promoting effect, a low dose (0.05~0.5 mM) exhibited an inhibitory effect, and a 5~25 There is no statistically significant difference between the mM concentration and the control protocol [1]. In animals lacking osteoprotegerin, bergapten (5-Methoxypsoralen) inhibits osteoporosis associated with diabetes via controlling the PI3K/AKT, JNK/MAPK, and NF-κB signaling pathways. It has also been demonstrated that bergamotene considerably reduces the synthesis of cytokines that promote inflammation. By preventing the activation of the PI3K/AKT, JNK/MAPK, and NF-κB signaling pathways as well as RANKL-RANK signaling, bergapten can prevent osteoclast differentiation and preserve trabecular integrity [2].
|
|---|---|
| ln Vivo |
The rat colon has a higher NAT metabolic activity than the stomach, and within 24 hours, bergamot lactone (5-Methoxypsoralen, 5-MOP) lowers the AF content in the stomach. The stomach and intestines have lower AAF concentrations. While DMSO (solvent) had an impact on AAF metabolism, bergamot lactone further boosted AAF metabolism and decreased both the 24-hour stomach and colonic AAF concentrations in comparison to the control regimen. A 24-to 72-hour timeframe is involved [1].
|
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion
Absorption was slow in volunteers after administration of capsule-form micronized bergamot lactone (peak serum concentration reached in 3.2 hours; elimination half-life approximately 1 hour). Intravenous injection in rabbits resulted in elimination half-lives of 1–2 minutes (α phase) and 15 minutes (β phase). 5-Methoxypsoralen exhibits a high binding affinity to serum proteins, with 98–99% binding. This high affinity leads to higher tissue concentrations. In the epidermis, it appears to bind to independent and non-interacting sites. Enrichment of 5-Methoxypsoralen in the epidermis was determined. It is concentrated in the human epidermis, with concentrations 10–500 times higher than in the surrounding buffer solution. Distribution among tissue components may explain its behavior. In young adult Hartley guinea pigs, a linear relationship was found between serum and epidermal concentrations of 5-methoxypsoralen, and observed skin phototoxicity correlated with serum 5-methoxypsoralen concentrations… For more complete data on the absorption, distribution, and excretion of 11 types of 5-methoxypsoralen, please visit the HSDB record page. Metabolic/Metabolic Substances Objective: To investigate the contribution of psoralen and bergamot lactone metabolites to psoralen toxicity. Methods: Metabolic reactions and toxic groups were predicted using computational chemistry based on the Derek and Meteor expert systems. Results: Based on first and second-stage biotransformations up to the third generation, a total of 15 metabolites of psoralen and bergamot lactone were predicted. Five toxic group substructures were found in psoralen, bergamot lactone, and their corresponding metabolites; one toxic group (resorcinol) was found only in bergamot lactone and its biotransformation products. Conclusion: Although the toxic effects of psoralen are well-known and documented, the role of its metabolites in this process is rarely reported. We believe this work contributes to a deeper understanding of which molecular substructures are involved in metabolism and toxicity induction processes, thereby guiding the development of more effective and less toxic vitiligo treatments. Multiple studies have shown that cytochrome P450 (P450) can convert furanocoumarin derivatives into active molecules, which can form covalent bonds with biomolecules. 5-Methoxypsoralen (5-MOP) is a natural furanocoumarin derived from plants in the Apiaceae family. This study investigated the effects of single nucleotide polymorphisms (SNPs) in the CYP2A13 gene on 5-MOP metabolism. We used wild-type CYP2A131 expressed in E. coli and its five variants: CYP2A134 (R101Q), CYP2A135 (F453Y), CYP2A136 (R494C), CYP2A138 (D158E), and CYP2A139 (V323L). High-performance liquid chromatography (HPLC) analysis showed that CYP2A131 can convert 5-MOP to 5-MOP dihydrodiol; the K(m) and V(max) values for this reaction were 1.44 ± 0.17 μM and 4.23 ± 0.36 nmol/(min × nmol P450), respectively. The conversion of 5-MOP to dihydrodiol suggests that the conversion of CYP2A13 leads to toxicity due to its covalent bonding with DNA or proteins. Most CYP2A13 variants metabolize 5-MOP; the Km values for CYP2A135, 6, 8, and 9 are 1.63 ± 0.12, 1.36 ± 0.10, 0.85 ± 0.09, and 0.58 ± 0.06 μM, respectively, and the Vmax values are 3.20 ± 0.13, 4.69 ± 0.13, 2.34 ± 0.07, and 1.84 ± 0.09 nmol/(min × nmol P450), respectively. However, no processing effect of CYP2A134 on 5-MOP was detected. Based on these data, we hypothesize that single nucleotide polymorphisms (SNPs) within the CYP2A13 gene affect the metabolism of 5-MOP in humans. Known metabolites of bergamot lactone include Unii-3abk64HG9O. Biological Half-Life After volunteers took the capsule-form micronized bergamot lactone, absorption was slow (peak serum concentration reached in 3.2 hours; elimination half-life was approximately 1 hour). When administered intravenously to rabbits, the elimination half-life was 1–2 minutes (α phase) and 15 minutes (β phase). |
| Toxicity/Toxicokinetics |
Toxicity Summary
Identification and Uses: 5-Methoxypsoralen (5-MOP) is a furanocoumarin. As a component of bergamot oil, 5-MOP is found in some perfumes, fragrances, sunscreens, and foods. It has been used to enhance the tanning effect in tanning products. 5-MOP, used in combination with UVA, is often used as a chemophototherapy agent for the treatment of psoriasis. Human Studies: Chemophototherapy is very effective in treating skin diseases such as psoriasis and can also be used for preventative "sclerotherapy" in patients with polymorphic light eruption. The most commonly used photosensitizer in oral chemophototherapy is furanocoumarin. In addition to phototoxic reactions caused by the photosensitizing activity of psoralen, side effects of oral psoralen include nausea, vomiting, headache, anxiety, and insomnia. Allergic reactions to 5-MOP have been reported. A 55-year-old female patient with psoriasis vulgaris received oral 5-MOP and UVA photochemotherapy. After 40 treatments over 3 months, she developed psoralen-induced hepatitis. 5-MOP causes chromosomal damage in human cells in vitro. Animal studies: When beagle dogs were orally administered 5-MOP at doses of 100 or 400 mg/kg daily (8 days), 60 mg/kg daily (28 days), or 48 mg/kg daily (26 weeks), delayed behavioral toxicities, including bullous dermatitis, bilateral keratitis, reduced food intake, and reduced weight gain, were observed in the highest dose group. Skin damage was reversible, while ocular damage was irreversible. Hepatomegaly, necrosis, and hepatitis were observed in the 48 mg/kg dose group. 5-MOP in combination with UVA and 12-O-tetradecanoylphorbol-13-acetate induced skin cancer in mice. Rats were orally administered 5-MOP daily (75 or 150 mg/kg) or excipient control. Compared with the control group, treated male animals showed significantly reduced pituitary volume, decreased sperm count per ejaculation, and reduced sperm count in the vas deferens and epididymis. Administration significantly increased testosterone levels and relative testicular weight, but did not directly affect testicular weight. Females mating with treated males required longer pregnancy times, while these males required more mating attempts. Female rabbits were orally administered 0, 70, or 560 mg/kg body weight daily during days 7–18 of gestation. The 560 mg/kg dose group showed maternal toxicity, and the rate of fetal malformations increased in a dose-dependent manner. 5-MOP forms a non-covalently bound complex with DNA in vitro under dark conditions. In Saccharomyces cerevisiae and Chinese hamster V79 cells, 5-MOP covalently binds to DNA in vitro under photosynthetic conditions. It can light-induced DNA strand cross-linking in vitro and in Chinese hamster V79 cells. 5-MOP has been reported to induce mutagenesis in Salmonella typhimurium TA100 (with or without metabolic activation) and Escherichia coli lac-z (ND160) alone. The combined use of 5-MOP and UVA reduced the survival rate of Bacillus subtilis and Escherichia coli repair-deficient mutants, while the addition of metabolic activators inhibited their lethal activity. Interactions Sunscreens containing 5-methoxypsoralen (5-MOP) are being commercially marketed to enhance sunbathing effects and sun protection efficacy. Sun System III (SS III) sunscreens containing 5-MOP and 20 joules/cm² of ultraviolet radiation (UVA) caused skin erythema and delayed pigmentation. Phototoxicity was not observed unless the output light from the solar simulator was filtered with water to reduce infrared radiation. This suggests that the skin phototoxicity response induced by 5-MOP plus UVA can be attenuated by heating. The use of phototoxic psoralen in sunscreens is inappropriate due to the increased risk of UV-induced skin cancer. Objective: This study aimed to investigate the potential effects of bergamot lactone on lipopolysaccharide (LPS)-mediated osteoclast formation, bone resorption, and osteoclast survival in vitro. Methods: RAW264.7 osteoclast precursor cells were treated with bergamot lactone (5, 20, 40 μmol/L) in the presence of LPS (100 ng/mL) for 72 hours. Osteoclastogenesis was identified by tartrate-resistant acid phosphatase (TRAP) staining, and the number of TRAP-positive multinucleated cells [TRAP(+) MNCs] in each well was counted. To investigate the effect of bergamot lactone on osteoclast bone resorption, RAW264.7 cells were treated with bergamot lactone for 6 days with LPS, and the bone resorption area was analyzed using Image Pro-Plus software. Next, we used Annexin V/propidium iodide (PI) double staining to detect apoptosis in RAW264.7 cells after 48 hours of bergamot lactone incubation by flow cytometry. Finally, we used Hoechst 33342 staining and Western blotting to observe osteoclast survival after 24 hours of bergamot lactone treatment. The results showed that bergamot lactone (5-40 μmol/L) inhibited LPS-induced osteoclast formation and bone resorption in a dose-dependent manner. Bergamot lactone treatment induced apoptosis in RAW264.7 osteoclast precursor cells in a dose-dependent manner. Furthermore, bergamot lactone significantly reduced the survival rate of mature osteoclasts, manifested by the appearance of apoptotic nuclei and activation of the apoptotic proteins caspase 3/9. Conclusion: These findings indicate that bergamot lactone effectively prevents LPS-induced osteoclast formation, bone resorption, and survival by inhibiting the apoptotic response of osteoclasts and their precursors. This study confirms that bergamot lactone is an inhibitor of osteoclast formation and bone resorption and provides evidence that bergamot lactone may be an alternative therapy for the prevention and treatment of inflammatory bone loss. Objective: Melanoma is an aggressive skin cancer. This study aimed to evaluate the effects of UVA radiation and psoralen: 5-methoxypsoralen (5-MOP) or 8-methoxypsoralen (8-MOP) on melanoma cell viability. Materials and Methods: Achromatic C32 and pigmented COLO829 human melanoma cell lines were exposed to increasing concentrations of psoralen (0.1–100 μM) under both UVA and UVA radiation conditions. Cell viability was assessed using the WST-1 assay. Results: Unlike 5-MOP, 8-MOP showed no cytotoxicity to either melanoma cell line. However, simultaneous exposure of C32 cells to both 8-MOP and UVA radiation resulted in significant cytotoxicity, with EC50 values of 131.0 μM (UVA dose: 1.3 J/cm²) and 105.3 μM (UVA dose: 2.6 J/cm²), respectively. UVA radiation significantly enhanced the cytotoxicity of 5-methoxypsoralen (5-MOP) on C32 and COLO829 cells—EC50 values were estimated at 22.7 or 7.9 μM (UVA dose: 1.3 J/cm²) and 24.2 or 7.0 μM (UVA dose: 2.6 J/cm²), respectively. Conclusion: In vitro experiments showed that melanoma cells exhibited high cytotoxicity after simultaneous exposure to psoralen and UVA radiation, suggesting the potential application value of PUVA therapy in in vivo for the treatment of melanoma. Objective: To investigate the hepatoprotective effect of 5-methoxypsoralen (5-MOP) and whether 5-MOP exhibits hepatotoxicity at protective doses. Methods: C57BL/6J mice were orally administered 5-MOP daily in the morning at doses of 12.5, 25, and 50 mg/kg body weight for 4 consecutive days, followed by subcutaneous injection of acetaminophen (APAP) at a dose of 500 mg/kg. A separate 5-MOP monotherapy group was established, in which mice were orally administered 5-MOP at a dose of 50 mg/kg body weight for 4 consecutive days, without APAP injection. Twenty-four hours after APAP administration, blood samples were collected from mice to measure serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), and lactate dehydrogenase (LDH) levels. The levels of malondialdehyde (MDA), reduced glutathione (GSH), and oxidized glutathione (GSSG) in liver tissue were also measured. Simultaneously, histopathological changes in the liver were observed. Results: Compared with the vector control group, serum ALT, AST, and LDH levels (IU/L) in the APAP group were significantly increased (8355±3940 vs 30±21, P<0.05; 6482±4018 vs 146±58, P<0.05; 24627±10975 vs 1504±410, P<0.05). Compared with the acetaminophen group, serum alanine aminotransferase (ALT) levels (IU/L) (1674±1810 vs 8355±3940, P<0.05; 54±39 vs 8355±3940, P<0.05; 19±9 vs 8355±3940, P<0.05), aspartate aminotransferase (AST) levels (IU/L) (729±685 vs 6482±4108, P<0.05; 187±149 vs 6482±4108, P<0.05; 141±12 vs 6482±4108, P<0.05), and lactate dehydrogenase (LDH) levels (IU/L) (7220±6317 vs 24627±141) were all significantly increased. The values of 10975 (P < 0.05); 1618±719 vs 24627±10975 (P < 0.05); and 1394±469 vs 24627±10975 (P < 0.05) were significantly reduced in all three 5-MOP pretreatment groups. 5-MOP pretreatment alleviated APAP-induced histopathological changes, including hepatocellular necrosis and inflammatory cell infiltration, in a dose-dependent manner. 5-MOP reduced MDA levels (nmol/mg) in a dose-dependent manner (0.98 +/- 0.45 vs 2.15 +/- 1.07, P > 0.05; 0.59 +/- 0.07 vs 2.15 +/- 1.07, P < 0.05; 0.47 +/- 0.06 vs 2.15 +/- 1.07, P < 0.05). 5-MOP pretreatment also increased the GSH/GSSG ratio (3.834±0.340 vs 3.306±0.282, P>0.05; 5.330±0.421 vs 3.306±0.282, P<0.05; 6.180±0.212 vs 3.306±0.282, P<0.05). In the group treated with 5-MOP only and not APAP, serum enzyme levels, liver histopathology, and MDA and GSH/GSSG ratios were all normal. Conclusion: 5-Methoxypsoralen (5-MOP) effectively protects C57BL/6J mice from APAP-induced hepatotoxicity, possesses antioxidant activity, and does not cause liver damage at protective doses. For more complete data on interactions of 5-methoxypsoralen (9 in total), please visit the HSDB record page. Non-human toxicity values: Mouse oral LD50: 8100 mg/kg body weight; Rat oral LD50: >30,000 mg/kg body weight; Guinea pig oral LD50: 9000 mg/kg body weight. |
| References |
|
| Additional Infomation |
According to an independent committee of scientific and health experts, 5-methoxypsoralen may be carcinogenic when used in combination with UVA therapy. It is a grayish-white microcrystalline powder or a yellow, fluffy solid. (NTP, 1992) 5-Methoxypsoralen is a 5-methoxyfuranocoumarin, a product of psoralen with a methoxy group substituted at the 5-position. It has hepatoprotective effects and is a plant metabolite. It belongs to the psoralen class of compounds, 5-methoxyfuranocoumarins, and organic heterocyclic tricyclic compounds. It is functionally related to psoralen. Bergamot lactone is being studied in the clinical trial NCT00533195 (a comparison of UVA1 phototherapy versus photochemotherapy for patients with severe generalized atopic dermatitis). Bergamot lactone has been reported in Caragana korshinskii, Angelica sinensis, and other organisms with relevant data. It is a linear furanocoumarin with phototoxic and anti-inflammatory properties, similar to methoxsalen. It is used in PUVA therapy for psoriasis.
See also: Parsley (part); Fennel (part); Angelica sinensis root (part)...See more... Therapeutic Use /Exploring Therapies/ Background: Psoralen combined with ultraviolet (UV) A (PUVA) therapy is the standard treatment for early-stage mycosis fungoides (MF). When 8-methoxypsoralen (8-MOP) is used in PUVA therapy, intolerance reactions such as nausea, vomiting, and headache are often caused. Objective: To investigate whether 5-methoxypsoralen (5-MOP) can be a safe and effective alternative to 8-MOP in PUVA therapy for mycosis fungoides (MF). Methods: A retrospective database search and medical record review were conducted to screen MF patients who received PUVA therapy at our hospital. These patients received either 5-MOP or 8-MOP as initial monotherapy. Between 1990 and 2004, 14 patients [7 males, 7 females; mean age 70 years, range 51–82 years; National Cancer Institute stage IA (n=6) and IB (n=8)] received 5-MOP treatment, and 24 patients [21 males, 3 females; mean age 58 years, range 28–89 years; stage IA (n=11), IB (n=12), and IIB (n=1)] received 8-MOP treatment. Results: 12 out of 14 patients (86%) in the 5-MOP group achieved complete remission with PUVA treatment, and 22 out of 24 patients (92%) in the 8-MOP group achieved complete remission. There were no significant differences between the two complete remission subgroups in terms of duration of PUVA treatment, number of treatments, or cumulative UVA dose. There were no significant differences between the two groups in relapse-free rate [8% (1/12) vs. 23% (5/22)] or time to relapse [17 months (range 4–31 months) vs. 14 months (range 4–33 months)]. Furthermore, in a subset of patients [26% (9/34)], maintenance therapy with PUVA using either 5-MOP or 8-MOP did not affect long-term relapse-free status. Conclusion: 5-methoxypsoralen (5-MOP) and 8-methoxypsoralen (8-MOP) have similar efficacy in PUVA therapy for mycosis fungoides (MF). 5-methoxypsoralen, when used in combination with UVA, is commonly used as a photochemotherapy drug for the treatment of psoriasis… Background: After oral administration, 5-methoxypsoralen (5-MOP) is comparable to 8-MOP in efficacy with PUVA therapy for psoriasis, with a lower incidence of acute skin side effects. Objective: We compared the efficacy of photochemotherapy with 5-MOP and 8-MOP bath solutions for the treatment of psoriasis. Methods: 22 patients underwent photosensitivity testing with 0.0003% 5-MOP or 8-MOP aqueous solutions. This study included a side-by-side comparison of 12 patients with palmar psoriasis and 10 patients with recurrent plaque psoriasis treated with either therapy. Results: The minimum phototoxic dose (MPD) was 2.8 ± 1.2 J/cm² in the 8-MOP group and 2.0 ± 1.2 J/cm² in the 5-MOP group (p < 0.01). Both therapies cleared lesions on the palms, but the 8-MOP group required a higher UVA dose (46.3 ± 21.0 J/cm² vs 30.2 ± 21.5 J/cm²; p < 0.01) and more sessions (21.0 ± 6.0 vs 17.0 ± 5.0; p = 0.02). Bath therapy-5-MOP-UVA was also more effective in treating plaque psoriasis (cumulative UVA dose: 56.8 ± 39.2 J/cm² vs 59.1 ± 27.9 J/cm²; number of sessions: 20.0 ± 5.7 vs 21.6 ± 4.7), but these differences were not statistically significant (p = NS). Compared with 8-MOP, patients in the 5-MOP group showed significant earlier onset of noticeable tanning (3.5 ± 0.5 weeks vs 4.4 ± 0.5 weeks; p < 0.01). Conclusion: Bath therapy-5-MOP-UVA has higher phototoxicity than bath therapy-8-MOP-UVA. It is more effective in treating palmar psoriasis, but its higher melanogenic activity appears to have an adverse effect on the treatment of plaque psoriasis. 5-Methoxypsoralen, a naturally occurring linear furanocoumarin, has been successfully used in combination with ultraviolet A (UVA) irradiation [psoralen combined with UVA (PUVA)] to treat psoriasis and vitiligo. In patients and volunteers, PUVA combined with 5-methoxypsoralen treatment resulted in a dose-dependent increase in skin photosensitivity. However, in individuals, the mean minimum phototoxic dose (MPD) of 5-methoxypsoralen was 30% to 50% higher than that of 8-methoxypsoralen; this indicates that 5-methoxypsoralen has lower photoactivity. In parallel-designed comparative clinical trials, psoriasis clearance rates of over 90% and 97% were achieved in patients receiving oral PUVA therapy with 5-methoxypsoralen (typically 1.2 mg/kg) or oral PUVA therapy with 8-methoxypsoralen (0.6 mg/kg), with similar patient numbers in both groups (60% to 77%). Generally, patients receiving 5-methoxypsoralen require a higher total UVA exposure to reach the treatment endpoint than those receiving 8-methoxypsoralen. However, in a small number of psoriasis patients receiving both treatments contralaterally, oral or topical PUVA therapy with 5-methoxypsoralen reached the study endpoint more quickly. Up to 56% of vitiligo patients experienced a pigment recovery rate exceeding 75% after treatment with 5-methoxypsoralen (oral or topical) combined with ultraviolet (lamp or sunlight) irradiation; the face and trunk were the most effective areas. Up to 16% of psoriasis patients treated with PUVA 5-methoxypsoralen experienced no response; in one trial, the non-response rate in vitiligo patients was as high as 22%. In one study, 7 (19%) vitiligo patients experienced lesion spread during treatment. The incidence and severity of adverse events were generally lower in patients treated with PUVA 5-methoxypsoralen 1.2 mg/kg than in patients treated with PUVA 8-methoxypsoralen 0.6 mg/kg. The most common short-term adverse events were nausea and/or vomiting, pruritus, and erythema; in clinical trials, these adverse events occurred approximately 2 to 11 times more frequently in patients treated with 8-methoxypsoralen than in patients treated with 5-methoxypsoralen. Hepatic adverse events following oral administration of this drug are uncommon. Currently, data on the long-term tolerability of PUVA 5-methoxypsoralen remain limited. However, no carcinogenicity was reported during a 14-year observation period in 413 patients with psoriasis. Conclusion: In patients with vitiligo or psoriasis, the lesion clearance rates of oral 5-methoxypsoralen or 8-methoxypsoralen combined with UVA irradiation are similar, but patients taking 5-methoxypsoralen generally require a higher total UV irradiation dose than those taking 8-methoxypsoralen. The incidence of short-term skin and gastrointestinal adverse reactions with 5-methoxypsoralen is significantly lower than with 8-methoxypsoralen, which is an advantage, but the long-term tolerability of 5-methoxypsoralen is not fully established. However, for appropriately selected patients, PUVA 5-methoxypsoralen therapy may be an alternative to first-line systemic treatment for vitiligo or psoriasis. Drug Warning It has been reported that 5-methoxypsoralen is the only active ingredient that causes benign dermatitis, which can cause patchy pigmentation on the face and neck… |
| Molecular Formula |
C12H8O4
|
|---|---|
| Molecular Weight |
216.1895
|
| Exact Mass |
216.042
|
| CAS # |
484-20-8
|
| Related CAS # |
Bergapten-d3;2749409-59-2
|
| PubChem CID |
2355
|
| Appearance |
White to off-white solid powder
|
| Density |
1.4±0.1 g/cm3
|
| Boiling Point |
412.4±45.0 °C at 760 mmHg
|
| Melting Point |
190-193 °C(lit.)
|
| Flash Point |
203.2±28.7 °C
|
| Vapour Pressure |
0.0±1.0 mmHg at 25°C
|
| Index of Refraction |
1.635
|
| LogP |
2
|
| Hydrogen Bond Donor Count |
0
|
| Hydrogen Bond Acceptor Count |
4
|
| Rotatable Bond Count |
1
|
| Heavy Atom Count |
16
|
| Complexity |
325
|
| Defined Atom Stereocenter Count |
0
|
| InChi Key |
BGEBZHIAGXMEMV-UHFFFAOYSA-N
|
| InChi Code |
InChI=1S/C12H8O4/c1-14-12-7-2-3-11(13)16-10(7)6-9-8(12)4-5-15-9/h2-6H,1H3
|
| Chemical Name |
4-methoxyfuro[3,2-g]chromen-7-one
|
| HS Tariff Code |
2934.99.9001
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
DMSO : ~20 mg/mL (~92.51 mM)
H2O : ~0.1 mg/mL (~0.46 mM) |
|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: 1 mg/mL (4.63 mM) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), suspension solution; with sonication.
For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 10.0 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. Solubility in Formulation 2: ≥ 1 mg/mL (4.63 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 10.0 mg/mL clear DMSO stock solution to 900 μL of corn oil and mix evenly. (Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 4.6256 mL | 23.1278 mL | 46.2556 mL | |
| 5 mM | 0.9251 mL | 4.6256 mL | 9.2511 mL | |
| 10 mM | 0.4626 mL | 2.3128 mL | 4.6256 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
|
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved