| Size | Price | Stock | Qty |
|---|---|---|---|
| 10mg |
|
||
| 25mg |
|
||
| 50mg |
|
||
| 100mg |
|
||
| 250mg |
|
||
| 500mg |
|
































Purity: ≥98%
| Targets |
hypoxia-inducible factor-α1 (HIF-α1); p53
|
|---|---|
| ln Vitro |
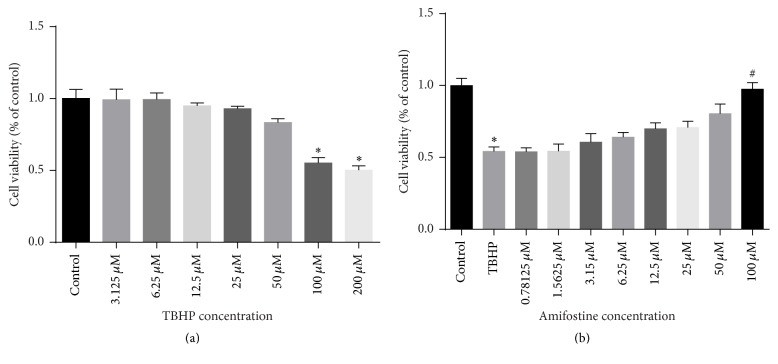
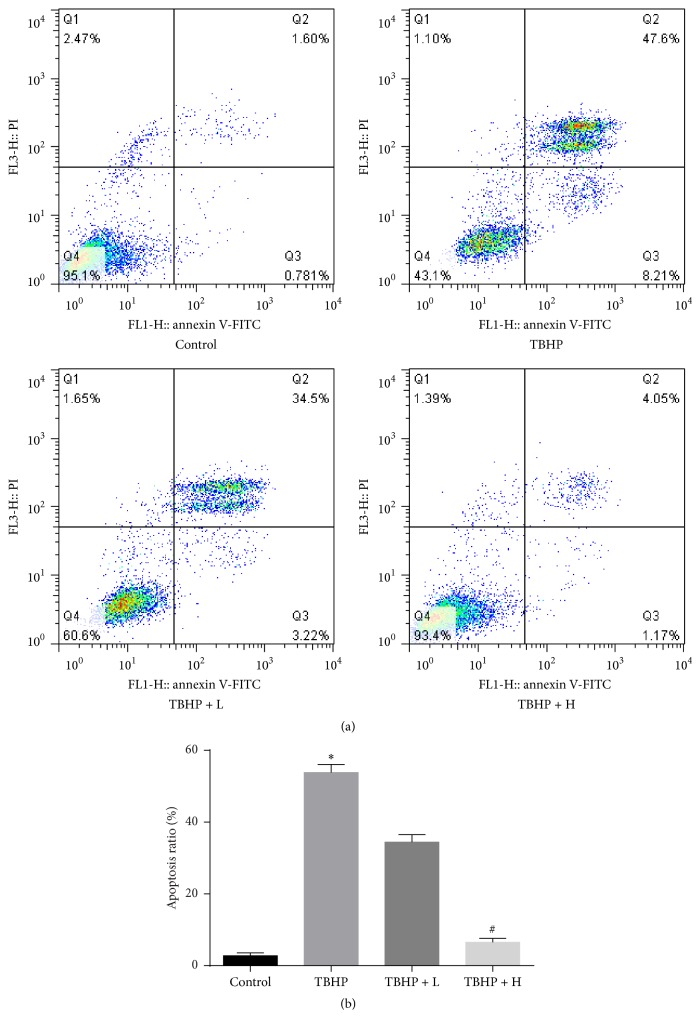
Amifostine (0.78125-100 μM, 24 h) dramatically lowers H9c2 cell apoptosis at a concentration of 100 μM and decreases tertiary tetrahydroperoxide (TBHP)-induced cell damage in a dose-wise manner [5].
|
| ln Vivo |
Amifostine (intravenous injection, 400 mg/kg, 4 hours) exerts a protective effect on myocardial I/R damage in male C57BL/6 mice [5].
|
| Enzyme Assay |
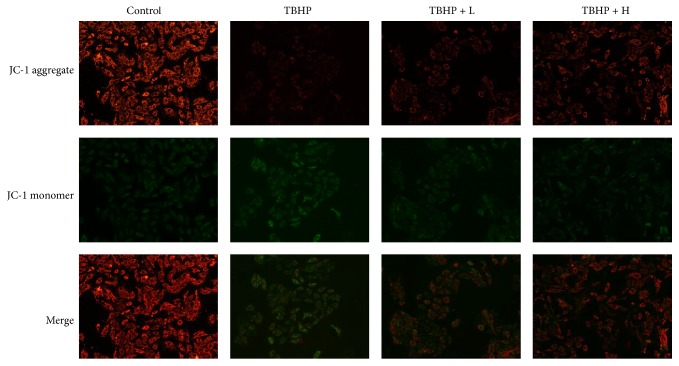
We used TBHP, a more stable chemical than H2O2, to induce oxidative stress. For measurement of ROS of the H9c2 cells, cells were incubated with 10 μmol/L ROS sensitive dye 2′,7′-dichloruoresceindiacetate (DCFH-DA) at 37°C for 20 min. ROS was detected by a flow cytometry sorter (BD Biosciences, San Jose, CA, USA) and quantified by BD FACS software. The above experiments were repeated three times. ΔΨm was measured using JC-1 staining; cells were seeded into Petri dishes. After treatment, the dishes were incubated in JC-1 staining solution (5 mg/ml) at 37°C for 20 min. Subsequently the staining cells were washed twice with JC-1 staining buffer; images were taken by a confocal laser scanning microscopy.[5]
|
| Cell Assay |
H9c2 cells were seeded into 96-well plates at a concentration of 5000 cells per well. The cells were pretreated with amifostine (0.78125, 1.5625, 3.125, 6.25, 12.5, 25, 50, and 100 μM) for 30 min before being exposure to tert-Butyl hydroperoxide (TBHP) for 12 h. The number of viable cells was evaluated by MTT assay. Briefly, MTT dye solution was added to each well and incubated for 4 h. The number of viable cells was measured by evaluating Absorbance at 490 nm. The MTT assay was repeated three times for consistency.[5]
|
| Animal Protocol |
Animal/Disease Models: Male C57BL/6 mice myocardial I/R injury[5]: 400 mg/kg
Route of Administration: intravenous (iv) (iv)injection; 4 hrs (hrs (hours)) Experimental Results: Attenuated cardiomyocyte apoptosis and diminished I/R-induced ROS production. Dramatically diminished the expression of cleaved caspase 3 and Bax, while enhancing the expression of SOD1, SOD2 and Bcl2. SOD activity was Dramatically increased and MDA levels were diminished. |
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion
Following intravenous injection of 150 mg/m² ethanol, renal excretion of the parent drug and its two metabolites was low within 10 seconds. Within one hour of administration, the average renal excretion of the parent drug, thiols, and disulfides was 0.69%, 2.64%, and 2.22% of the administered dose, respectively. Measurable concentrations of the active free thiol metabolite were detected in bone marrow cells 5 to 8 minutes after intravenous injection. It is currently unknown whether amifostine or its metabolites are distributed into breast milk. The drug is primarily eliminated through rapid metabolism and tissue absorption. ...Studies of single subcutaneous injections of amifostine in rats showed no drug accumulation in either normal or tumor tissues, with peak concentrations of WR-1065 in tumors slightly above...the limit of quantitation during treatment... This study investigated the pharmacokinetics of the cytoprotective agent amifostine (Ethyol®; WR 2721) and its major metabolites (WR 1065 and disulfide) in participating patients in two Phase I clinical trials of carboplatin or cisplatin in combination with amifostine. Patients received one or three doses of amifostine (740 or 910 mg/m²). The single or first dose was administered via intravenous infusion over 15 minutes prior to chemotherapy. The remaining two infusions were administered at 2 hours and 4 hours, respectively. Amifostine was rapidly cleared from plasma, at least in part due to its rapid conversion to WR 1065. A biphasic decline was observed, with a final half-life of 0.8 hours. The final half-life of the active metabolite WR 1065 cleared from plasma was 7.3 ± 3.6 hours. The short initial half-life of WR 1065 can be attributed to its rapid absorption in tissues and the formation of disulfides. The final half-life of the disulfides ranged from 8.4 to 13.4 hours and was detectable for at least 24 hours after treatment. They may serve as an exchange pool for WR 1065. In multiple-dose regimens, peak concentrations of amifostine did not accumulate at the end of each 15-minute infusion. For WR 1065, an increasing trend in peak levels was observed [C1,max: 47.5 +/- 11.9 uM, C2,max: 79.0 +/- 13.2 uM, C3,max: 84.8 +/- 15.1 uM, (n = 6)], while a slightly decreasing trend was observed in disulfide peak levels [C1,max: 184.2 +/- 12.6 uM, C2,max: 175.0 +/- 23.7 uM, C3,max: 166.0 +/- 17.2 uM, (n = 6)]. This latter finding may suggest that disulfide bond formation has reached saturation, or that the absorption or elimination of WR 1065 has been altered, leading to increased plasma and tissue WR 1065 levels after repeated administrations of amifostine. Metabolism/Metabolites Amifostine is rapidly dephosphorylated in tissues by alkaline phosphatase to an active free thiol metabolite, which is then further converted to a less active disulfide bond metabolite. Amifostine is rapidly dephosphorylated in tissues by alkaline phosphatase to an active free thiol metabolite, which is then further converted to a less active disulfide bond metabolite. No unchanged amifostine was detected in urine within one hour following intravenous infusion at doses of 740 to 910 mg/m² body surface area over 15 minutes, or rapid intravenous injection at doses of 150 mg/m² body surface area over 10 seconds. Amifostine, disulfide metabolites, and thiol metabolites accounted for only 0.69%, 2.22%, and 2.64% of the dose, respectively. This study investigated the metabolism of the radioprotective compound WR-2721 (amifostine; S-2-(3-aminopropylamino)ethyl thiophosphate) in Balb/c mice. …It is known that radiation protection requires the conversion of the parent drug into its free thiol metabolite WR-1065 in cultured cells. Since the metabolite of WR-1065 may participate in the protective effect, and thiols are highly metabolically active molecules, we investigated the metabolism of WR-2721 using electrochemical detection-high performance liquid chromatography (EC-HPLC). The main findings of this study are as follows: 1) WR-2721 is rapidly cleared from the blood. Thirty minutes after administration, the blood concentration of the parent drug decreased tenfold from the maximum observed value at 5 minutes. 2) WR-1065 rapidly appears in the perchloric acid (PCA) soluble fraction of normal tissues. Ten minutes after administration, the highest concentrations of WR-1065 in the liver and kidneys were 965 and 2195 μmol/kg, respectively; while the highest concentrations in the heart and small intestine at 30 minutes were 739 and 410 μmol/kg, respectively. 3) WR-1065 accumulated at a lower rate in the PCA soluble fraction of two experimental tumors than in other tissues. Biological half-life 8 minutes Approximately 8 minutes; less than 10% of amifostine remained in plasma 6 minutes after administration. This study investigated the pharmacokinetics of the cytoprotective agent amifostine (Ethyol®; WR 2721) and its major metabolites (WR 1065 and disulfide) in participating patients in two Phase I clinical trials of carboplatin or cisplatin in combination with amifostine. Patients received a single or triple dose of amifostine (740 or 910 mg/m²). The single or first dose was administered via intravenous infusion over 15 minutes prior to chemotherapy. The remaining two infusions were administered at 2 hours and 4 hours, respectively. Amifostine was rapidly cleared from plasma, at least in part attributable to its rapid conversion to WR 1065. A biphasic decline was observed, with a final half-life of 0.8 hours. The final half-life of the active metabolite WR 1065 cleared from plasma is 7.3 ± 3.6 hours. The short initial half-life of WR 1065 can be attributed to its rapid absorption in tissues and the formation of disulfides. The final half-life of the disulfides is 8.4–13.4 hours and they are detectable for at least 24 hours after treatment. They may serve as an exchange pool for WR 1065. |
| Toxicity/Toxicokinetics |
Rats (intraperitoneal injection): LD50: 418 mg/kg
Rats (intramuscular injection): LD50: 396 mg/kg Mice (oral injection): LD50: 842 mg/kg Mice (intraperitoneal injection): LD50: 321 mg/kg Mice (intravenous injection): LD50: 557 mg/kg Mice (intramuscular injection): LD50: 514 mg/kg Dogs (intravenous injection): LD50: 279 mg/kg Interactions Repeated oral administration of melatonin and ascorbic acid (200 mg/kg) 30 minutes before treatment with γ-phosphatase (γ-fos) reduced its cumulative toxicity. Under these conditions, succinic acid (100 mg/kg) was ineffective. The cumulative time to death for 50% of animals treated with γ-phosphate alone or in combination with melatonin, ascorbic acid, and succinic acid were 3.08 days, 4.29 days, 4.06 days, and 2.97 days, respectively. PMID: 15455115 Amifostine may cause temporary hypotension; antihypertensive medications or other medications that may cause hypotension should be discontinued 24 hours before administration of amifostine; patients receiving antihypertensive treatment that cannot be discontinued should not receive amifostine. Antidote and Emergency Treatment Immediately take first aid measures: Ensure adequate decontamination has been performed. If the patient stops breathing, begin artificial respiration immediately, preferably using a ventilator on demand, bag-valve-mask, or simple breathing mask, and follow the training instructions. Perform cardiopulmonary resuscitation if necessary. Immediately flush contaminated eyes with running water. Do not induce vomiting. If vomiting occurs, tilt the patient forward or place them in the left lateral decubitus position (head down if possible) to maintain an open airway and prevent aspiration. Keep the patient calm and maintain normal body temperature. Seek immediate medical attention. /Class A and Class B Poisoning/ Basic Treatment: Establish a patent airway (use an oropharyngeal or nasopharyngeal airway if necessary). Suction if necessary. Observe for signs of respiratory failure and provide assisted ventilation if necessary. Administer oxygen via a non-invasive ventilation mask at a flow rate of 10 to 15 liters per minute. Monitor for pulmonary edema and treat as necessary… Monitor for shock and treat as necessary… Anticipate seizures and treat as necessary… If eyes are contaminated, flush with water immediately. During transport, continuously flush each eye with 0.9% saline… Do not use emetics. In case of ingestion, rinse mouth and dilute with 5 mL/kg to 200 mL of water, provided the patient is able to swallow, has a strong gag reflex, and does not drool… After decontamination, cover skin burns with a dry, sterile dressing… /Class A and B Poisons/ Advanced Treatment: For patients with altered mental status, severe pulmonary edema, or severe respiratory distress, consider oropharyngeal or nasopharyngeal endotracheal intubation to control the airway. Positive pressure ventilation with a bag-valve-mask may be effective. Consider medical treatment for pulmonary edema… Consider the use of a beta-agonist (such as salbutamol) for severe bronchospasm… Monitor heart rhythm and treat arrhythmias if necessary… Initiate intravenous infusion of 5% glucose solution (SRP: “Keep it patent,” minimum flow rate). If signs of hypovolemia appear, use 0.9% normal saline or lactated Ringer's solution. Use fluids with caution in cases of hypotension with signs of hypovolemia. Watch for signs of fluid overdose… Use diazepam or lorazepam for seizures… Use promecaine hydrochloride to assist eye irrigation… /Toxins A and B/ Toxicity Data Rat (intraperitoneal injection): LD50: 418 mg/kg Rat (intramuscular injection): LD50: 396 mg/kg Mouse (oral): LD50: 842 mg/kg Mouse (intraperitoneal injection): LD50: 321 mg/kg Mouse (intravenous injection): LD50: 557 mg/kg Mouse (intramuscular injection): LD50: 514 mg/kg Dog (intravenous): LD50: 279 mg/kg Interactions Repeated oral administration of melatonin and ascorbic acid (200 mg/kg) 30 minutes prior to treatment with γ-phosphatase (γ-fos) reduced its cumulative toxicity. Under these conditions, succinic acid (100 mg/kg) was ineffective. The cumulative time to death in 50% of animals treated with γ-phosphate monotherapy or in combination with melatonin, ascorbic acid, and succinate was 3.08 days, 4.29 days, 4.06 days, and 2.97 days, respectively. Amifostine may temporarily cause hypotension; antihypertensive drugs or other medications that may cause hypotension should be discontinued 24 hours before administration of amifostine; patients receiving antihypertensive therapy that cannot be discontinued should not receive amifostine. Non-human toxicity values: Mouse intraperitoneal LD50 700 mg/kg /amifostine monohydrate/ |
| References | |
| Additional Infomation |
Therapeutic Uses
Radioprotective Agents Amifostine is indicated for reducing cumulative nephrotoxicity caused by repeated cisplatin use in patients with advanced ovarian cancer. /Included in the US product label/ Amifostine is indicated for reducing cumulative nephrotoxicity caused by repeated cisplatin use in patients with advanced non-germ cell solid tumors. /Not included in the US product label/ Amifostine is indicated for reducing the risk of moderate to severe xerostomia in patients receiving postoperative radiotherapy for head and neck tumors whose radiation field includes most of the parotid gland. /Included in the US product label/ For more complete data on the therapeutic uses of amifostine (8 types), please visit the HSDB record page. Drug Warnings Although the incidence of hypocalcemia during amifostine cytoprotective therapy is low, serum calcium levels should be monitored in patients at risk of hypocalcemia, such as those with nephrotic syndrome or those receiving multiple amifostine treatments, and calcium supplementation should be given as needed. Because nausea and/or vomiting are common and can be severe during amifostine treatment, effective antiemetic therapy (e.g., intravenous corticosteroids such as dexamethasone and 5-HT3 receptor antagonists) should be administered before and during amifostine treatment. Depending on the emetogenicity of concurrent chemotherapy or radiotherapy, additional antiemetics may be necessary. Furthermore, fluid balance should be closely monitored in patients receiving highly emetogenic chemotherapy. Patients should be closely monitored during and after intravenous amifostine administration for anaphylactic reactions, including rare anaphylactic shock associated with cardiac arrest. In the event of an acute hypersensitivity reaction, the infusion should be permanently stopped immediately. The manufacturer notes that epinephrine and other appropriate emergency measures should be readily available for immediate management of such events. For infusions lasting less than 5 minutes, blood pressure should be monitored at least before the infusion begins and immediately after the infusion ends, and continued as necessary. If hypotension occurs and the amifostine infusion needs to be interrupted, the patient should be placed in a head-down, feet-up position, and a 0.9% sodium chloride solution should be infused via another vein. For more complete data on amifostine (9 of 9), please visit the HSDB record page. Pharmacodynamics: Amifostine is an organothiophosphate cytoprotective agent indicated for reducing the cumulative nephrotoxicity caused by repeated cisplatin use in patients with advanced ovarian cancer or non-small cell lung cancer, and for reducing the incidence of moderate to severe xerostomia in patients receiving postoperative radiotherapy for head and neck tumors. Amifostine is a prodrug that is dephosphorylated in tissues by alkaline phosphatase to a pharmacologically active free thiol metabolite, which is believed to reduce the cumulative nephrotoxicity of cisplatin and mitigate the toxic effects of radiation on normal oral tissues. Because the concentration of amifostine and its metabolites in healthy cells is 100 times higher than in tumor cells, healthy cells are preferentially protected. |
| Molecular Formula |
C5H21N2O6PS
|
|---|---|
| Molecular Weight |
268.27
|
| Exact Mass |
214.054
|
| Elemental Analysis |
C, 28.03; H, 7.06; N, 13.08; O, 22.41; P, 14.46; S, 14.97
|
| CAS # |
20537-88-6
|
| Related CAS # |
112901-68-5 (trihydrate); 20537-88-6 (free); 59178-37-9 (sodium); 63717-27-1 (monohydrate)
|
| PubChem CID |
2141
|
| Appearance |
White to off-white solid powder
|
| Density |
1.4±0.1 g/cm3
|
| Boiling Point |
441.7±51.0 °C at 760 mmHg
|
| Melting Point |
160-161ºC
|
| Flash Point |
220.9±30.4 °C
|
| Vapour Pressure |
0.0±2.3 mmHg at 25°C
|
| Index of Refraction |
1.555
|
| LogP |
-1.68
|
| Hydrogen Bond Donor Count |
4
|
| Hydrogen Bond Acceptor Count |
6
|
| Rotatable Bond Count |
7
|
| Heavy Atom Count |
12
|
| Complexity |
152
|
| Defined Atom Stereocenter Count |
0
|
| SMILES |
OP(SCCNCCCN)(O)=O
|
| InChi Key |
JKOQGQFVAUAYPM-UHFFFAOYSA-N
|
| InChi Code |
InChI=1S/C5H15N2O3PS/c6-2-1-3-7-4-5-12-11(8,9)10/h7H,1-6H2,(H2,8,9,10)
|
| Chemical Name |
2-((3-Aminopropyl)amino)-ethanethiol, dihydrogen phosphate ester (9CI)
|
| Synonyms |
Apaetp; AU-95722; YM-08310;NSC 296961; S 8744; Ethyol; Sapep; Aminopropylaminoethyl thiophosphate; NSC-296961; WR 2721; YM 08310; Ethiofos; Gammaphos;
|
| HS Tariff Code |
2934.99.03.00
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
H2O : ~100 mg/mL (~466.81 mM)
DMF : 1 mg/mL (~4.67 mM) DMSO :< 1 mg/mL |
|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: 100 mg/mL (466.81 mM) in PBS (add these co-solvents sequentially from left to right, and one by one), clear solution; with sonication (<60°C).
(Please use freshly prepared in vivo formulations for optimal results.) |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 3.7276 mL | 18.6379 mL | 37.2759 mL | |
| 5 mM | 0.7455 mL | 3.7276 mL | 7.4552 mL | |
| 10 mM | 0.3728 mL | 1.8638 mL | 3.7276 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
| NCT Number | Recruitment | interventions | Conditions | Sponsor/Collaborators | Start Date | Phases |
| NCT00130143 | Completed | Drug: Ethyol (Amifostine) | Head and Neck Cancer Lung Cancer |
The Dale & Frances Hughes Cancer Center | 2003-06 | Not Applicable |
| NCT00601198 | Terminated | Drug: Amifostine | Colorectal Cancer | University of Cincinnati | 2006-10 | Phase 2 |
| NCT00078845 | Completed | Drug: Amifostine | Breast Cancer Lung Cancer Neurotoxicity Ovarian Cancer |
M.D. Anderson Cancer Center | 2004-05 | Phase 2 |
| NCT05167370 | Terminated | Drug: Amifostine | Brain Tumors Solid Tumors |
Children's Hospital Medical Center, Cincinnati | 2010-12-13 | Phase 2 |
| NCT00003048 | Completed | Drug: Amifostine Trihydrate | Myelodysplastic Syndromes | M.D. Anderson Cancer Center | 1997-06-05 | Phase 2 |
|
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved





























 COA
COA